Comprehensive motor neuron disease guide covering critical warning signs, proven care strategies, and essential support resources for patients and families.
Introduction
Motor neuron disease (MND) represents a group of progressive neurological conditions that attack the nerve cells controlling voluntary muscle movement. These devastating disorders gradually rob people of their ability to walk, speak, swallow, and eventually breathe, while typically leaving intellect and cognitive function intact. Though currently incurable, understanding motor neuron disease—its early warning signs, progression patterns, and comprehensive care strategies—empowers patients and families to maximize quality of life, access crucial support resources, and maintain dignity throughout this challenging journey.
Understanding Motor Neuron Disease
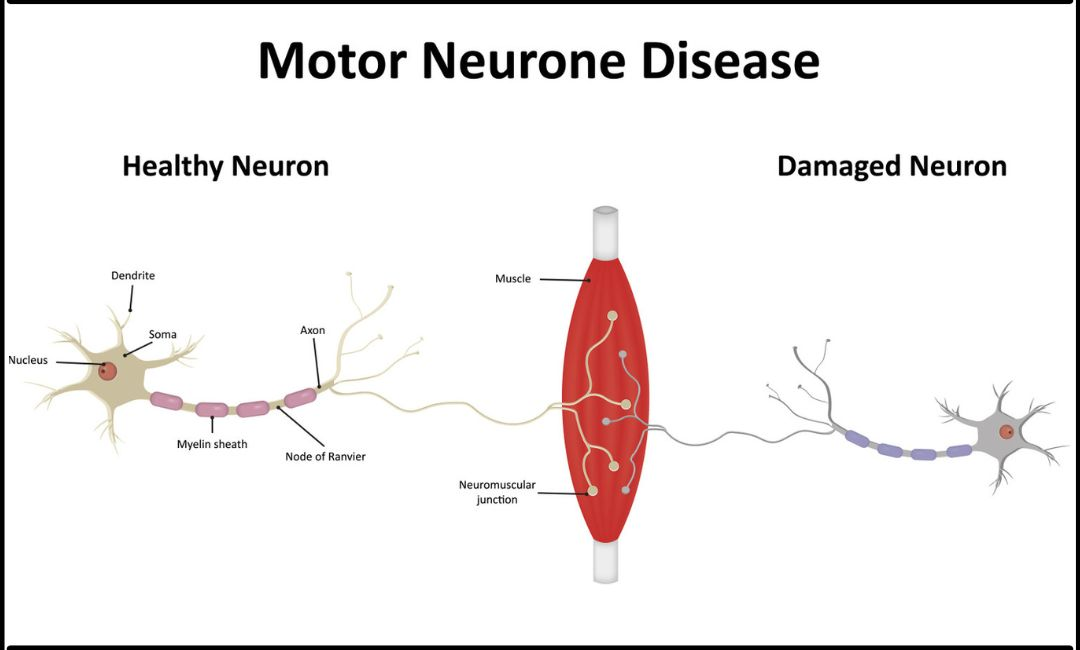
Motor neurons are specialized nerve cells responsible for transmitting signals from your brain and spinal cord to muscles throughout your body. These signals enable every voluntary movement—from walking and talking to breathing and swallowing. Motor neuron disease occurs when these critical nerve cells progressively deteriorate and die, disrupting communication between your nervous system and muscles.
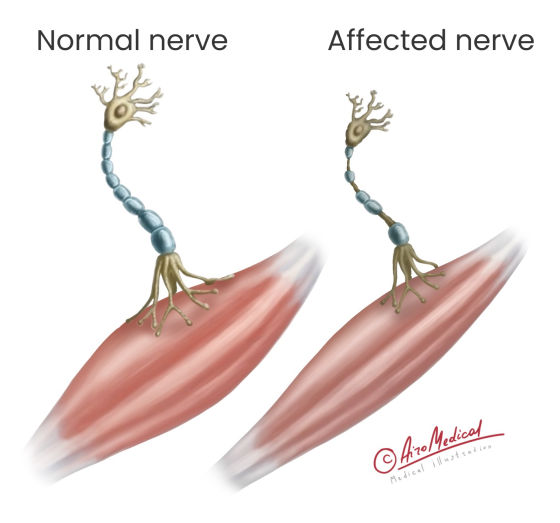
As motor neurons degenerate, muscles gradually weaken, waste away (atrophy), and eventually become paralyzed. The disease typically spares sensory neurons (those responsible for touch, taste, sight, smell, and hearing) and generally doesn’t affect bowel or bladder control. Most importantly, cognitive function remains intact in the majority of cases, meaning people remain mentally alert while trapped in progressively weakening bodies.
According to the ALS Association, approximately 5,000 people in the United States are diagnosed with ALS—the most common form of motor neuron disease—annually, with about 30,000 Americans living with the condition at any time.
Types of Motor Neuron Disease
Motor neuron disease encompasses several distinct conditions affecting different motor neuron populations:
Amyotrophic Lateral Sclerosis (ALS): Also called Lou Gehrig’s disease after the famous baseball player diagnosed with it, ALS is the most common and severe form of MND. It affects both upper motor neurons (in the brain) and lower motor neurons (in the spinal cord), causing rapidly progressive muscle weakness, atrophy, and paralysis. Most people with ALS survive 3 to 5 years after diagnosis, though approximately 10 percent live 10 years or longer.
Progressive Bulbar Palsy (PBP): This form primarily affects motor neurons controlling muscles used for speaking, chewing, and swallowing. It typically begins with difficulty speaking and swallowing, often progressing to affect other body areas. PBP may occur alone or develop as part of ALS progression.
Progressive Muscular Atrophy (PMA): This rare form affects only lower motor neurons in the spinal cord, causing slow progressive muscle weakness and wasting. PMA generally progresses more slowly than ALS and has better prognosis, though it can eventually affect respiratory muscles.
Primary Lateral Sclerosis (PLS): The rarest form, PLS affects only upper motor neurons, causing stiffness and weakness in legs initially, then progressing to arms and bulbar muscles. PLS progresses more slowly than ALS and doesn’t typically shorten lifespan.
Spinal Muscular Atrophy (SMA): Unlike other forms primarily affecting adults, SMA is inherited and typically begins in childhood. It results from defective or missing SMN1 genes essential for motor neuron survival.
Recognizing Early Warning Signs
Motor neuron disease symptoms develop gradually, often so subtly that early signs are dismissed as normal aging, overexertion, or minor injuries. Recognizing these early indicators facilitates prompt diagnosis and care planning.
Initial Symptoms
Muscle Weakness: The earliest and most common symptom, weakness typically begins in one limb—often hands, arms, legs, or feet. You might notice difficulty gripping objects, dropping things frequently, tripping or stumbling while walking, or struggling with buttons, zippers, or doorknobs. This progressive weakness spreads to other body regions over time.
Muscle Twitching (Fasciculations): Involuntary muscle twitches, particularly visible under skin surface, occur commonly in MND. While fasciculations can result from many benign causes, persistent widespread twitching combined with weakness warrants medical evaluation.
Muscle Cramps and Stiffness: Painful muscle cramps, particularly in hands and feet, may occur frequently. Muscle stiffness (spasticity) makes movement difficult and uncomfortable.
Speech Changes: Difficulty articulating words (dysarthria), slurred speech, nasal quality to voice, or speaking more slowly may indicate bulbar involvement affecting muscles controlling speech.
Swallowing Difficulties (Dysphagia): Trouble swallowing liquids or solid foods, choking easily, or feeling food stuck in throat signals bulbar muscle weakness. Similar to how other neurological conditions like epilepsy require careful symptom monitoring, tracking swallowing difficulties helps guide appropriate interventions.
Fatigue: Profound exhaustion disproportionate to activity level results from muscles working harder to compensate for weakness.
Progressive Symptoms
As disease advances, additional symptoms emerge:
Respiratory Problems: Weakening respiratory muscles cause shortness of breath, difficulty breathing when lying flat, morning headaches from inadequate nighttime breathing, and frequent respiratory infections.
Weight Loss: Muscle wasting, swallowing difficulties, and increased caloric needs from labored breathing contribute to progressive weight loss.
Emotional Lability: Uncontrollable laughing or crying inappropriate to the situation (pseudobulbar affect) occurs in some patients, resulting from disease affecting brain regions controlling emotional expression.
Cognitive Changes: While most people maintain normal cognition, approximately 15 percent develop frontotemporal dementia affecting behavior, personality, and judgment. Similar to challenges faced with dementia in general, these changes require specialized management approaches.
Communication Difficulties: As speech becomes impossible, patients require alternative communication devices to maintain connection with loved ones and caregivers.
What Causes Motor Neuron Disease?
The exact causes of most MND cases remain unknown, though research has identified several contributing factors:
Genetic Factors: Approximately 5 to 10 percent of ALS cases are familial (inherited), resulting from genetic mutations passed through families. Several genes have been identified, including SOD1, C9orf72, and TARDBP. Most cases are sporadic, occurring without family history, though genetic factors may still contribute to susceptibility.
Environmental Factors: Various environmental exposures have been investigated as potential triggers including heavy metals, pesticides, certain chemicals, and head trauma, though no definitive causal relationships have been established.
Oxidative Stress: Damage from free radicals may harm motor neurons, though whether this is cause or consequence remains unclear.
Glutamate Toxicity: Excessive glutamate (a neurotransmitter) may damage motor neurons through overstimulation.
Immune System Dysfunction: Some evidence suggests immune system abnormalities may contribute to motor neuron damage.
Protein Misfolding: Abnormal protein accumulation in motor neurons appears common in MND, potentially disrupting cellular function.
According to the National Institute of Neurological Disorders and Stroke, most cases likely result from complex interactions between genetic predisposition and environmental factors.
Diagnosing Motor Neuron Disease
No single test definitively diagnoses MND. Diagnosis involves ruling out other conditions while documenting progressive motor neuron degeneration.
Clinical Examination: Neurologists perform detailed examinations assessing muscle strength, tone, and bulk; reflexes (typically hyperactive in MND); fasciculations and muscle twitching; coordination and balance; and speech and swallowing function.
Electromyography (EMG): This test measures electrical activity in muscles, detecting abnormalities characteristic of motor neuron damage. Small needles inserted into muscles record electrical patterns during rest and contraction.
Nerve Conduction Studies: These tests measure how well nerves transmit electrical signals, helping distinguish MND from other neuromuscular conditions.
MRI Scans: Brain and spinal cord imaging rules out other conditions mimicking MND symptoms, such as tumors, herniated discs, or multiple sclerosis.
Blood and Urine Tests: Laboratory studies exclude other conditions causing similar symptoms, including thyroid disorders, vitamin deficiencies, or Lyme disease.
Genetic Testing: For patients with family history, genetic testing identifies known mutations, though negative results don’t exclude MND.
Diagnosis often takes months as doctors monitor symptom progression and rule out alternative explanations. This delay can be frustrating but ensures diagnostic accuracy.
Treatment and Management Strategies
While no cure exists for motor neuron disease, comprehensive multidisciplinary care significantly improves quality of life and may extend survival.
Medications
Riluzole (Rilutek): The first FDA-approved ALS medication, riluzole modestly slows disease progression, extending survival by several months. It works by reducing glutamate levels, potentially protecting motor neurons from damage.
Edaravone (Radicava): This newer medication may slow functional decline in some patients by reducing oxidative stress. It’s administered intravenously or orally.
Symptom Management Medications: Various drugs address specific symptoms including muscle relaxants for spasticity and cramps, anticholinergic medications for excessive saliva, antidepressants for depression and pseudobulbar affect, and pain medications for discomfort.
Respiratory Support
As breathing muscles weaken, respiratory interventions become essential:
Non-Invasive Ventilation (NIV): BiPAP machines deliver pressurized air through masks, supporting breathing during sleep or rest. NIV significantly improves quality of life and extends survival.
Mechanical Ventilation: For patients who choose it, tracheostomy with mechanical ventilation provides full breathing support, potentially extending life considerably. This decision requires careful consideration of personal values and quality of life preferences.
Cough Assist Devices: These machines help clear secretions by simulating cough, reducing pneumonia risk.
Nutritional Support
Maintaining adequate nutrition becomes challenging as swallowing difficulties progress. Strategies include modifying food textures to ease swallowing, working with speech therapists on safe swallowing techniques, and eventually placing feeding tubes (gastrostomy) for direct nutritional delivery. Early feeding tube placement, before severe weight loss occurs, improves outcomes. These nutritional approaches align with healthy eating principles adapted for specific medical needs.
Physical and Occupational Therapy
Therapists play crucial roles in maintaining function and independence. Physical therapy preserves muscle strength and flexibility, manages spasticity, prevents contractures, and recommends appropriate workout routines adapted to declining abilities. Occupational therapy provides adaptive equipment for daily activities, suggests home modifications for safety and accessibility, teaches energy conservation techniques, and helps maintain independence longer.
Speech and Communication Support
As speech deteriorates, speech-language pathologists recommend communication devices ranging from simple letter boards to sophisticated computer-based systems using eye-tracking technology, teach techniques for maximizing remaining speech ability, and advise on swallowing strategies and nutritional modifications.
Psychological and Emotional Support
MND’s progressive nature profoundly impacts mental health for both patients and families. Accessing mental health support through counseling helps process grief and adjustment, addresses depression and anxiety common in chronic illness, facilitates advance care planning discussions, and provides family support and caregiver education. Managing stress and anxiety through techniques like mindfulness improves emotional wellbeing throughout the disease journey.
Maximizing Quality of Life
Despite MND’s progressive nature, many people maintain remarkable quality of life through comprehensive care and support:
Maintain Social Connections: Stay engaged with family and friends through adaptive communication methods. Social isolation worsens depression and reduces quality of life.
Pursue Meaningful Activities: Continue enjoying hobbies and interests as abilities allow, adapting activities to current capabilities rather than abandoning them entirely.
Plan Ahead: Address practical matters including advance directives specifying treatment preferences, financial planning for care costs, legal documents like power of attorney, and discussions about end-of-life wishes with loved ones.
Join Support Groups: Connecting with others facing similar challenges provides emotional support, practical advice, and reduces feelings of isolation. Many organizations offer online communities for those with mobility limitations.
Optimize Sleep: Quality rest becomes increasingly important yet challenging. Implementing sleep better strategies, positioning aids, and respiratory support improves sleep quality.
Address Pain and Discomfort: Work closely with healthcare providers to manage pain, muscle cramps, and other uncomfortable symptoms. Adequate symptom control dramatically improves quality of life.
Embrace Assistive Technology: Wheelchairs, communication devices, home modifications, and other adaptive equipment maintain independence and connection to the world.
Frequently Asked Questions About Motor Neuron Disease
Is motor neuron disease hereditary?
Most MND cases (90 to 95 percent) are sporadic, occurring without family history. However, 5 to 10 percent of cases are familial, resulting from inherited genetic mutations. If you have a family member with MND, discuss genetic counseling with healthcare providers to understand your risk.
Does motor neuron disease affect thinking and memory?
Most people with MND maintain normal cognitive function throughout the disease course. However, approximately 15 percent develop cognitive changes, typically affecting executive function, behavior, and personality rather than memory. About 5 percent develop frontotemporal dementia requiring additional care considerations.
How quickly does motor neuron disease progress?
Progression varies significantly between individuals. ALS typically progresses rapidly, with most people surviving 3 to 5 years from diagnosis, though some live much longer. Other forms like PLS progress more slowly over decades. Factors affecting progression include disease type, age at onset, site of symptom onset, and overall health.
Can motor neuron disease be prevented?
Currently, no known prevention strategies exist for MND. Maintaining overall health through regular exercise, balanced nutrition, avoiding smoking, and minimizing head trauma supports general neurological health but doesn’t specifically prevent MND.
Are there any promising treatments in development?
Significant research efforts focus on developing new MND treatments. Ongoing clinical trials investigate gene therapies, stem cell approaches, new medications targeting different disease mechanisms, and combination therapies. While no breakthroughs have yet emerged, research continues advancing understanding and treatment possibilities.
How does motor neuron disease affect life expectancy?
Prognosis varies by disease type and individual factors. ALS has the most serious prognosis, with median survival of 3 to 5 years from diagnosis, though approximately 10 percent of patients live 10 years or more. PLS progresses much more slowly and typically doesn’t shorten lifespan. Respiratory support, nutritional management, and comprehensive multidisciplinary care can extend survival and improve quality of life.
What support resources are available for patients and families?
Numerous organizations provide information, support, and resources including the ALS Association offering patient services, support groups, and equipment loans; MND Association providing comprehensive information and support networks; local ALS clinics offering multidisciplinary care coordination; and online communities connecting patients and caregivers worldwide. Social workers help navigate insurance, disability benefits, and care services.
Supporting Someone With Motor Neuron Disease
If your loved one has been diagnosed with MND, your support plays a vital role in their quality of life:
Educate Yourself: Understanding the disease, its progression, and care needs helps you provide better support and anticipate challenges.
Communicate Openly: Encourage honest discussions about feelings, fears, wishes, and practical matters. Listen without judgment and validate their emotions.
Maintain Normalcy: Treat your loved one as you always have, recognizing they remain the same person despite physical changes. Avoid overprotecting or infantilizing them.
Support Independence: Help them maintain autonomy in decision-making and activities as long as safely possible. Balance assistance with preserving dignity and control.
Care for Yourself: Caregiving is physically and emotionally exhausting. Prioritize your own health, accept help from others, take regular breaks, and seek support through counseling or caregiver groups. You cannot pour from an empty cup.
Celebrate Small Victories: Focus on what remains possible rather than what’s been lost. Find joy in present moments and create meaningful memories.
Moving Forward With Courage and Hope

Motor neuron disease is devastating, challenging patients and families in profound ways. Yet countless individuals demonstrate remarkable courage, resilience, and grace while facing this condition. While current treatments remain limited, comprehensive multidisciplinary care, adaptive technologies, and strong support systems enable many people to maintain meaningful quality of life despite progressive disability.
Research continues advancing understanding of MND mechanisms and developing potential therapies. Clinical trials offer hope for future treatments that may slow progression, improve symptoms, or ultimately cure these conditions. Every research participant, advocacy effort, and fundraising initiative moves science closer to breakthroughs that will change outcomes for future generations.
Whether you’re newly diagnosed, caring for someone with MND, or supporting a friend through this journey, remember that you’re not alone. Extensive support networks, medical expertise, and communities of others facing similar challenges stand ready to help. With comprehensive care, open communication, and determination to maximize quality of life each day, it’s possible to face motor neuron disease with dignity, purpose, and hope.

