Here’s a number worth knowing: nearly half of adults in the United States have high or borderline-high cholesterol, according to data from the CDC. Yet cholesterol is one of those topics most people feel they sort-of understand, until they sit down with their doctor and realise the numbers on their lab report raise more questions than answers. What exactly is LDL? Why does your doctor care about it? And does eating eggs really matter?
Cholesterol is not the villain it was once made out to be. Your body actually needs it, to build cell membranes, produce hormones, and synthesise vitamin D. The problem arises when certain forms of cholesterol accumulate in the wrong places and in the wrong amounts, silently damaging blood vessels over years and decades.
In this post we cover everything you need to understand about cholesterol: what it is, how the different types are measured and interpreted, what drives levels up or down, and what 2026’s landmark new guidelines mean for how it’s now treated. Whether your doctor has flagged your numbers or you simply want to stay ahead of your heart health, this guide gives you the knowledge to act.
WHAT IS CHOLESTEROL AND WHY DOES YOUR BODY NEED IT?
Cholesterol is a waxy, fat-like substance found in every cell of your body. It is essential for life. Your body uses cholesterol to build and maintain cell membranes, produce sex hormones (oestrogen, testosterone) and stress hormones (cortisol), synthesise vitamin D from sunlight, and create bile acids that help you digest dietary fats.
Your liver produces about 75–80% of the cholesterol in your body. The remaining 20–25% comes from the food you eat, primarily animal-based products. This is why dietary changes alone have limits: even if you ate no cholesterol at all, your liver would continue producing it.
Because cholesterol is a fat and blood is water-based, cholesterol cannot travel through the bloodstream on its own. Instead, it is packaged into carriers called lipoproteins, which are combinations of fat and protein that act as transport vehicles. It is the type and quantity of these lipoproteins, not cholesterol itself, that determines your cardiovascular risk.
→ Related: [link to post on how the cardiovascular system works
THE DIFFERENT TYPES: LDL, HDL, VLDL AND TRIGLYCERIDES
A standard lipid panel measures four key values. Here is what each one means.
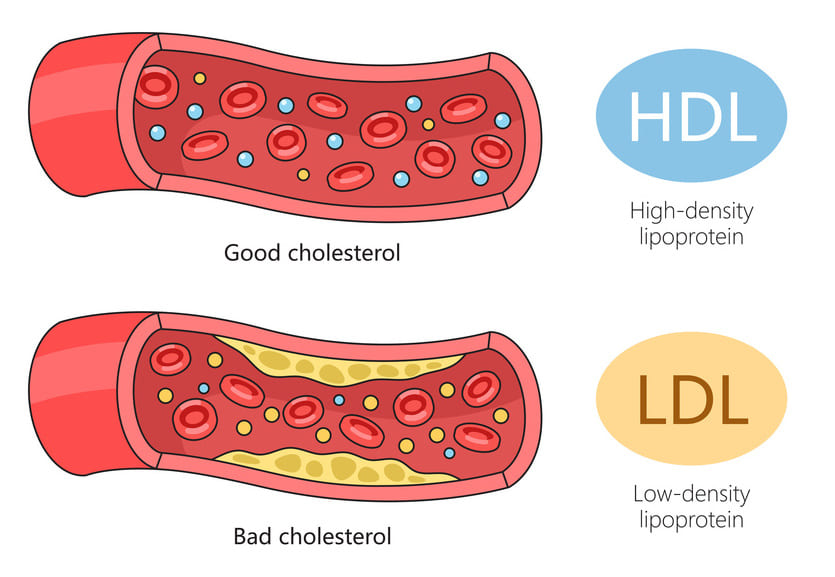
LDL-C: “Bad” Cholesterol
LDL (low-density lipoprotein) is the primary transporter of cholesterol from the liver to the rest of the body. When LDL levels are elevated, excess cholesterol can deposit in the walls of arteries, forming plaques, a process called atherosclerosis. Over time, these plaques narrow arteries and raise the risk of heart attack and stroke.
LDL-C (the amount of cholesterol carried by LDL particles) is the single most important number in cholesterol management. The 2026 ACC/AHA Dyslipidemia Guideline, the most comprehensive update to U.S. cholesterol guidance in nearly a decade, released in 2026, restores explicit LDL-C treatment goals based on individual cardiovascular risk:
- Very high risk (existing heart disease or equivalent): LDL-C goal < 55 mg/dL (1.4 mmol/L)
- High risk: LDL-C goal < 70 mg/dL (1.8 mmol/L)
- Moderate risk: LDL-C goal < 100 mg/dL (2.6 mmol/L)
- Lower risk: LDL-C < 116 mg/dL (3.0 mmol/L)
These goals were also affirmed in the 2025 ESC/EAS focused update on cholesterol management, published August 2025, suggesting strong international consensus.
HDL-C: “Good” Cholesterol
HDL (high-density lipoprotein) performs the reverse journey, transporting excess cholesterol from the arteries back to the liver, where it is broken down and removed. Higher HDL-C is generally associated with lower cardiovascular risk.
- Desirable HDL-C: ≥ 60 mg/dL (1.55 mmol/L)
- Low HDL-C (a risk factor): < 40 mg/dL in men, < 50 mg/dL in women
Importantly, the relationship between HDL and heart disease is more nuanced than the “good cholesterol” label suggests. Clinical trials attempting to raise HDL pharmacologically have not consistently reduced heart disease risk. What matters most is still lowering LDL, raising HDL is considered secondary by current guidelines.
Triglycerides
Triglycerides are the most common type of fat in your blood. After you eat, calories your body does not need immediately are converted to triglycerides and stored in fat cells. Elevated triglycerides, particularly in combination with low HDL or high LDL, raise the risk of atherosclerotic cardiovascular disease (ASCVD) and can cause pancreatitis at very high levels.
- Normal: < 150 mg/dL
- Borderline high: 150–199 mg/dL
- High: 200–499 mg/dL
- Very high (pancreatitis risk): ≥ 500 mg/dL
The 2026 ACC/AHA guideline reinforces that statin therapy remains the cornerstone of treatment for elevated triglycerides as a cardiovascular risk reducer, with additional TG-lowering therapies considered when levels exceed 1,000 mg/dL.
Non-HDL Cholesterol and Lp(a)
Two values increasingly used alongside LDL-C are non-HDL cholesterol (total cholesterol minus HDL, capturing all atherogenic lipoproteins) and Lp(a) (lipoprotein a), a genetically determined lipoprotein that significantly raises cardiovascular risk independently of LDL. The 2025 ESC/EAS update specifically highlights Lp(a) as a key risk factor and endorses emerging therapies targeting it.
Non-HDL-C goals mirror LDL-C goals plus 30 mg/dL (per the 2026 ACC/AHA guideline):
- Very high risk: non-HDL-C < 85 mg/dL
- High risk: non-HDL-C < 100 mg/dL
WHAT CAUSES HIGH CHOLESTEROL?
High cholesterol, technically called dyslipidaemia or hypercholesterolaemia, has multiple contributing causes. Understanding which applies to you is important for choosing the right treatment approach.
Lifestyle Factors
Diet is the most directly modifiable factor:
- Saturated fats (found in red meat, full-fat dairy, coconut and palm oil) raise LDL-C more than almost any other dietary component.
- Trans fats (partially hydrogenated oils, now largely banned in the U.S. but still present in some processed foods) both raise LDL and lower HDL, the worst possible combination.
- Refined carbohydrates and added sugars primarily raise triglyceride levels.
- Dietary cholesterol (eggs, shellfish) have less impact on blood cholesterol than previously believed. Current guidelines no longer impose a numerical cap on dietary cholesterol for the general population, though limiting saturated fat remains the priority.
- Physical inactivity lowers HDL and raises triglycerides.
- Obesity, particularly central (abdominal) obesity, is associated with raised LDL, raised triglycerides, and reduced HDL.
- Smoking lowers HDL-C and damages arterial walls, accelerating atherosclerosis.
- Excess alcohol raises triglyceride levels.
Genetic Factors
Familial hypercholesterolaemia (FH) is the most clinically important genetic cholesterol disorder, affecting approximately 1 in 250 people worldwide. It is caused by mutations in genes involved in LDL receptor function, resulting in dramatically elevated LDL-C from birth. People with untreated FH face a 20-fold higher risk of premature heart disease. FH is severely underdiagnosed, the majority of people with the condition are unaware they have it.
If you have a family history of heart disease at a young age (before 55 in men, before 65 in women), or very high total cholesterol despite a healthy lifestyle, ask your doctor about FH screening.
→ Related: [link to genetic testing and family planning
Medical Conditions and Medications
Several conditions can raise cholesterol levels secondary to the underlying disease:
- Hypothyroidism (underactive thyroid)
- Type 2 diabetes
- Chronic kidney disease
- Polycystic ovary syndrome (PCOS)
- Liver disease
Certain medications, including corticosteroids, antipsychotics, some blood pressure drugs, and antiretroviral therapy for HIV can also adversely affect lipid levels. Always inform your doctor about all medications and supplements you take when discussing cholesterol.
UNDERSTANDING YOUR CHOLESTEROL TEST
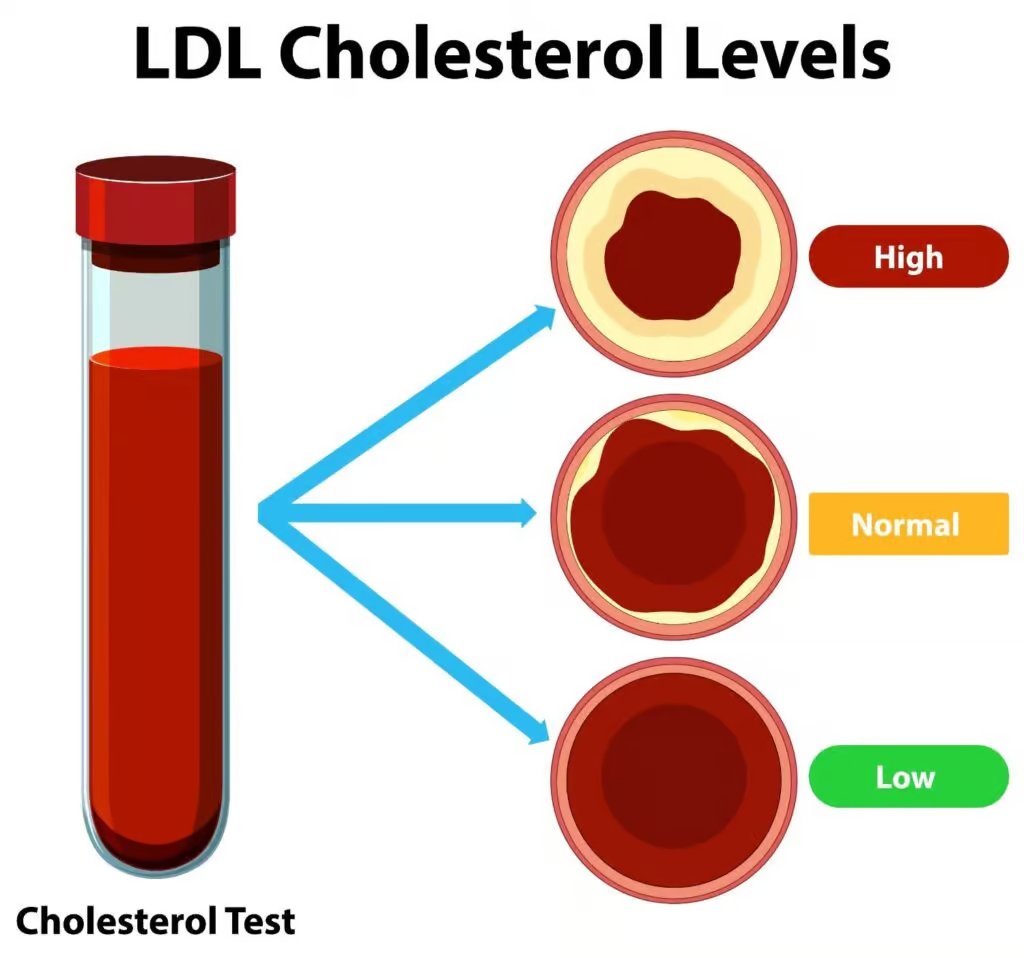
Cholesterol is measured through a lipid panel (also called a lipid profile), typically a simple fasting blood test. The 2026 ACC/AHA guideline promotes universal lipid testing across the lifespan, starting in childhood for those with family history of early heart disease or FH, and for all adults from age 20 onwards.
| Measurement | Desirable Level (adults) |
| Total cholesterol | < 200 mg/dL |
| LDL-C | Varies by risk (see above) |
| HDL-C | ≥ 60 mg/dL (protective) |
| Non-HDL-C | < 130 mg/dL (low risk) |
| Triglycerides | < 150 mg/dL |
| Lp(a) | < 75 nmol/L (< 30 mg/dL) |
A critical shift in the 2026 guidelines: rather than applying a single universal LDL target to everyone, treatment goals are now calibrated to your overall 10-year ASCVD risk, calculated using validated tools like the AHA PREVENT calculator (updated 2024) that incorporates total cholesterol, HDL, age, blood pressure, diabetes status, and other factors.
Your numbers do not exist in isolation. A person with an LDL of 130 mg/dL but no other risk factors may need no medication. A person with the same LDL plus a history of heart attack needs aggressive treatment. Context is everything.
→ Related: [link to post on understanding blood test results
LIFESTYLE CHANGES THAT ACTUALLY MOVE THE NEEDLE
Before any medication is considered, lifestyle change is the universal first step and for lower-risk individuals, it may be sufficient. Here is what the evidence supports.
Diet
The dietary pattern with the strongest evidence for improving lipid profiles is one that:
- Replaces saturated fats with unsaturated fats (olive oil, avocados, nuts, oily fish), this can lower LDL-C by 10–15%
- Emphasises soluble fibre (oats, barley, pulses, fruit, vegetables), 5–10g of soluble fibre daily can reduce LDL-C by a further 3–5%
- Includes plant sterols and stanols (found in fortified spreads and some dairy products), at doses of 2g/day, these block intestinal cholesterol absorption and can lower LDL-C by 7–10%
- Reduces refined carbohydrates and added sugar to manage triglycerides
- Limits alcohol to recommended levels
The Mediterranean diet and the DASH diet both align with these principles and have robust evidence for cardiovascular protection.
NOTE ON EGGS: Current guidance has moved away from strict limits on dietary cholesterol. Moderate egg consumption (up to one per day) does not appear to raise cardiovascular risk for most people, though those with diabetes or FH may still benefit from moderation. As always, what you pair with your eggs matters more than the eggs themselves.
Exercise
Regular aerobic exercise raises HDL-C, lowers triglycerides, and can modestly reduce LDL-C. Guidelines recommend at least 150 minutes of moderate-intensity aerobic activity per week (e.g. brisk walking, cycling, swimming) or 75 minutes of vigorous activity.
Even modest activity, a 30-minute walk five days a week is sufficient to produce lipid benefits. Resistance training provides additional metabolic benefits, particularly for triglycerides and blood sugar.
Weight Management and Smoking Cessation
Losing 5–10% of body weight can produce meaningful improvements in LDL-C, triglycerides, and HDL-C, even without specific dietary changes. Quitting smoking raises HDL-C within weeks and reduces ASCVD risk substantially over time.
→ Related: link to post on how to quit smoking
→ Related: [link to stress management strategies
MEDICATION: STATINS AND THE NEW OPTIONS IN 2026
When lifestyle change alone is insufficient, or when cardiovascular risk is high enough to require immediate pharmacological intervention, medication is recommended. The treatment landscape has expanded significantly.
Statins: The Foundation
Statins (atorvastatin, rosuvastatin, simvastatin, and others) are the most prescribed class of cholesterol medication worldwide and remain the cornerstone of treatment in both the 2026 ACC/AHA and 2025 ESC/EAS guidelines. They work by inhibiting HMG-CoA reductase, the enzyme responsible for cholesterol production in the liver, reducing LDL-C by 30–55% depending on the dose and agent.
Statins have an extraordinary evidence base: decades of randomised controlled trials consistently demonstrate that LDL-C lowering with statins reduces the risk of heart attack, stroke, and cardiovascular death. The 2026 ACC/AHA guideline calls for follow-up lipid panels 4–12 weeks after starting or changing statin therapy, then every 6–12 months.
Common concerns about statins:
- Muscle aches (myalgia): the most frequently reported side effect, affecting up to 10% of users in observational studies. Severe muscle damage (rhabdomyolysis) is very rare. Switching statins or adjusting dose often resolves the issue.
- Liver effects: routine liver enzyme monitoring is no longer recommended in current guidelines, as clinically significant liver injury from statins is extremely rare.
- Diabetes risk: statins modestly increase fasting blood glucose. For most high-risk patients, the cardiovascular benefit far outweighs this small risk.
Non-Statin Therapies
When statins alone do not achieve LDL-C goals, or in patients who cannot tolerate statins, the 2026 ACC/AHA guideline recommends the following add-on therapies:
- Ezetimibe; an oral tablet that blocks intestinal cholesterol absorption; lowers LDL-C by an additional 15–20% on top of statins; well-tolerated and inexpensive
- Bempedoic acid; a newer oral agent that inhibits cholesterol synthesis upstream of statins and can be used by statin-intolerant patients; endorsed in both the 2026 ACC/AHA and 2025 ESC/EAS guidelines
- PCSK9 monoclonal antibodies (alirocumab / Praluent, evolocumab / Repatha), injectable therapies given every 2–4 weeks that can lower LDL-C by 50–60% on top of maximal statin therapy; primarily used in very high-risk patients and FH
- Inclisiran; a twice-yearly injectable RNA-based therapy targeting PCSK9; approved in multiple countries; the 2026 guideline notes that cardiovascular outcomes trial data are still being evaluated
For elevated Lp(a), new therapies including pelacarsen and olpasiran (small interfering RNA agents) are in late-stage trials and expected to transform management of this genetically determined risk factor within the next few years.
→ Related: link to post on gene therapy and the future of medicine
WHAT’S NEW: THE 2026 ACC/AHA DYSLIPIDAEMIA GUIDELINE
The 2026 ACC/AHA/Multisociety Guideline on the Management of Dyslipidaemia, a major international collaboration involving 13 professional organisations, represents the most significant update to U.S. cholesterol guidance since 2018. Here are the key changes and what they mean for patients:
★ RESTORED LDL-C TREATMENT GOALS: The 2018 guideline controversially moved away from specific LDL-C targets. The 2026 guideline reverses this, restoring explicit numerical LDL-C goals stratified by cardiovascular risk. Most clinicians welcome this return to clarity.
★ UNIVERSAL LIPID TESTING: The guideline now advocates measuring lipids across the lifespan, including in children at risk, to identify and treat dyslipidaemia early, before cardiovascular damage accumulates.
★ Lp(a) GIVEN FORMAL PROMINENCE: Lp(a) screening is now strongly recommended at least once in every adult’s lifetime as part of cardiovascular risk assessment.
★ EXPANDED NON-STATIN OPTIONS: Bempedoic acid is now formally recommended as a front-line non-statin option, reflecting the maturation of its evidence base since the 2018 guideline.
★ CHILDREN AND YOUNG ADULTS: New specific guidance addresses lipid management in paediatric and young adult populations, recognising that atherosclerosis begins in childhood.
These changes represent a meaningful tightening of cardiovascular prevention ambitions and give both patients and clinicians clearer targets to work toward.
ADDRESSING THE CONTROVERSIES, EGGS, STATINS, AND DIETARY FAT
Few topics in nutrition generate more heated debate than cholesterol. Here is where the evidence actually stands.
“Statins are dangerous / a conspiracy.” Statins are among the most studied medications in the history of medicine. The weight of evidence from hundreds of randomised controlled trials and meta-analyses, involving hundreds of thousands of patients, consistently demonstrates their safety and effectiveness. Fringe claims that statins cause widespread harm are not supported by the scientific consensus and can actively harm patients who stop effective medication as a result.
“Saturated fat doesn’t cause heart disease.” This claim, popularised in certain media and nutrition circles, misrepresents the evidence. While the diet–heart relationship is genuinely complex, and replacing saturated fat with refined carbohydrates does not appear to reduce risk, replacing saturated fat with unsaturated fat (particularly polyunsaturated fat) does reduce cardiovascular risk. The American Heart Association and the 2026 ACC/AHA guideline maintain recommendations to limit saturated fat.
“Cholesterol is not the cause, inflammation is.” This is a false dichotomy. Both LDL-C and inflammation contribute to atherosclerosis. LDL-C lowering reduces events even in people with low inflammation markers. Addressing inflammation in addition to LDL-C, not instead of it, is the emerging evidence-based approach.
KEY TAKEAWAYS
✦ Cholesterol is essential, but the wrong types in the wrong amounts silently damage blood vessels over years. LDL-C (“bad”) is the primary target; HDL-C (“good”) and triglycerides matter too.
✦ The 2026 ACC/AHA Dyslipidaemia Guideline has restored clear LDL-C treatment goals based on individual risk. Very high-risk patients now have a target of < 55 mg/dL, a more demanding standard than previous guidance.
✦ Lifestyle changes, reducing saturated fat, increasing fibre and unsaturated fats, regular exercise, not smoking, and weight management, can meaningfully lower LDL-C and should be the starting point for anyone with elevated levels.
✦ Statins remain the most evidence-backed medication for LDL-C lowering. Non-statin options including ezetimibe, bempedoic acid, and PCSK9 inhibitors provide powerful additional tools when statins alone are insufficient.
✦ Know your numbers, and know what they mean in context. A single LDL reading is not enough; your overall 10-year cardiovascular risk determines what treatment, if any, you need.
CLOSING
Cholesterol management has never been more evidence-based or more nuanced. The arrival of the 2026 ACC/AHA guideline, with its restored treatment targets, universal testing push, and expanded therapeutic toolkit, gives both patients and clinicians an unprecedented level of clarity about what to aim for and how to get there.
The most important step you can take today is simply to know your numbers. Ask your doctor for a full lipid panel at your next visit, and ask them to explain what your results mean in the context of your overall cardiovascular risk. High cholesterol is one of the most treatable risk factors for the leading cause of death worldwide. That makes it one of the most powerful levers you have over your long-term health.