Struggling with ear pain? Learn the key symptoms of Otitis Media, effective treatments, and proven prevention steps to stop middle ear infections for good.
Introduction
Few childhood ailments cause as much distress as middle ear infections—the inconsolable crying of a toddler pulling at their ear, fever spikes in the middle of the night, and the helpless frustration of parents seeking relief for their suffering child. Otitis media, the medical term for middle ear infection, affects the majority of children before their third birthday and remains one of the most common reasons for pediatric doctor visits and antibiotic prescriptions. While predominantly affecting young children, adults also develop these painful infections. Understanding otitis media—its causes, symptoms, treatment options, and prevention strategies—empowers parents and patients to navigate these infections effectively, make informed treatment decisions, and reduce recurrence risk.
What Is Otitis Media? Understanding Middle Ear Infections
Otitis media refers to inflammation and infection of the middle ear—the air-filled space behind the eardrum containing tiny vibrating bones (ossicles) that transmit sound. This space connects to the back of the throat through the Eustachian tube, a narrow passage that normally equalizes pressure and drains fluid from the middle ear.

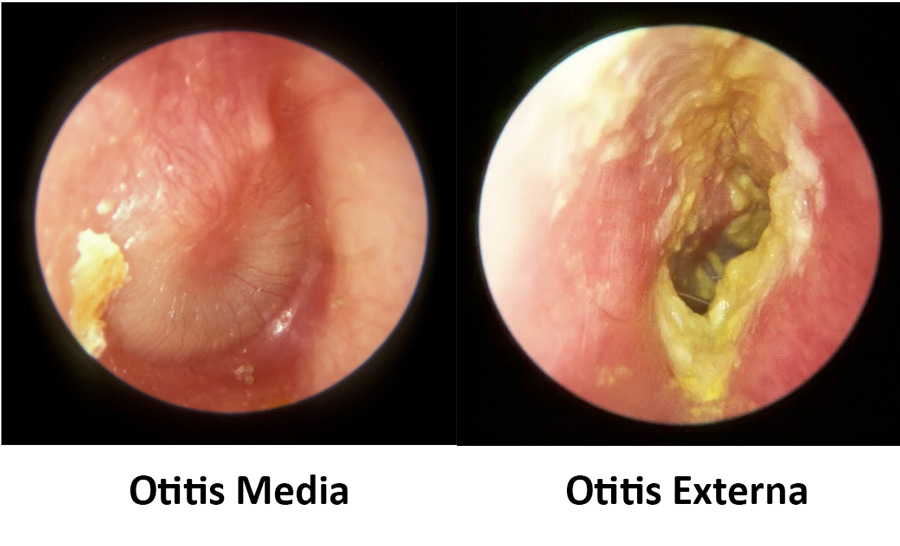
When bacteria or viruses infect the middle ear, inflammation develops, fluid accumulates, and pressure builds behind the eardrum, causing the characteristic pain and symptoms of otitis media. Unlike outer ear infections (otitis externa) affecting the ear canal, middle ear infections occur in the space behind the intact eardrum.
Types of Otitis Media:
Acute Otitis Media (AOM): Sudden onset infection with rapid symptom development, typically following upper respiratory infections. The most common type, usually bacterial.
Otitis Media with Effusion (OME): Also called “glue ear,” this condition involves fluid trapped in the middle ear without active infection. May follow AOM or develop independently, causing hearing difficulties without significant pain.
Chronic Otitis Media with Effusion: Persistent fluid accumulation lasting three months or longer, often causing ongoing hearing problems.
Chronic Suppurative Otitis Media: Long-term infection with persistent ear drainage through perforated eardrum, requiring specialized treatment.
Recurrent Acute Otitis Media: Three or more separate AOM episodes within six months, or four or more within one year, indicating underlying predisposing factors.
Recognizing Otitis Media Symptoms: Warning Signs
Symptoms vary by age, with young children unable to verbalize discomfort clearly:
Infants and Young Children:
- Ear pulling or tugging: Children instinctively pull at painful ears
- Excessive crying or irritability: Particularly worse when lying down as pressure increases
- Difficulty sleeping: Pain intensifies in horizontal position
- Fever: Often 100-104°F (37.8-40°C)
- Fluid drainage from ear: Yellow, clear, or bloody discharge indicating possible eardrum perforation
- Difficulty hearing or responding to sounds: Fluid blocks sound transmission
- Loss of balance or clumsiness: Middle ear affects balance
- Loss of appetite: Chewing and swallowing change pressure, causing pain
- Fussiness during feeding: Particularly bottle-fed babies
Older Children and Adults:
- Ear pain (otalgia): Sharp, throbbing, or aching pain in affected ear(s)
- Feeling of fullness or pressure in ear: Sensation of “plugged” ear
- Muffled hearing or temporary hearing loss: Fluid blocks sound waves
- Dizziness or vertigo: Middle ear dysfunction affects balance
- Fever and general malaise: Though less common in adults
- Headache
- Ear drainage: If eardrum ruptures (often provides pain relief)
- Difficulty sleeping on affected side
Similar to recognizing symptoms in respiratory infections, early identification of otitis media enables prompt treatment preventing complications.
Causes and Risk Factors: Why Middle Ear Infections Develop
Primary Causes:
Bacterial Infections: Account for most acute otitis media cases. Common culprits include:
- Streptococcus pneumoniae
- Haemophilus influenzae
- Moraxella catarrhalis
Viral Infections: Respiratory viruses (rhinovirus, RSV, influenza, adenovirus) cause upper respiratory infections that predispose to secondary bacterial middle ear infections. Viruses directly infect middle ear in some cases.
Eustachian Tube Dysfunction: The critical factor linking respiratory infections to otitis media. When Eustachian tubes become swollen or blocked from colds, allergies, or sinus infections, fluid cannot drain properly, creating ideal conditions for bacterial growth.
Risk Factors in Children:
Age: Infants and toddlers (6 months to 2 years) face highest risk due to:
- Shorter, more horizontal Eustachian tubes that drain poorly
- Immature immune systems
- Frequent upper respiratory infections
Daycare Attendance: Close contact with many children increases respiratory infection exposure.
Bottle-Feeding Position: Feeding babies lying flat allows milk to flow into Eustachian tubes.
Pacifier Use: Beyond age 6 months increases otitis media risk, particularly during sleep.
Secondhand Smoke Exposure: Irritates and inflames Eustachian tubes and respiratory passages, similar to how air pollution damages respiratory health.
Lack of Breastfeeding: Breast milk provides antibodies protecting against infections during first six months.
Family History: Genetic susceptibility increases risk.
Allergies: Nasal and throat inflammation from allergies affects Eustachian tube function.
Cleft Palate or Craniofacial Abnormalities: Structural differences impair Eustachian tube function.
Immune Deficiencies: Conditions weakening immune responses increase infection susceptibility.
Risk Factors in Adults:
- Chronic sinusitis or nasal congestion
- Allergies
- Smoking or smoke exposure
- Enlarged adenoids
- Recent upper respiratory infections
- Frequent air travel or altitude changes
Diagnosis: How Doctors Identify Otitis Media
Medical History:
Your doctor asks about symptoms, duration, previous ear infections, risk factors, and treatments tried.
Physical Examination:
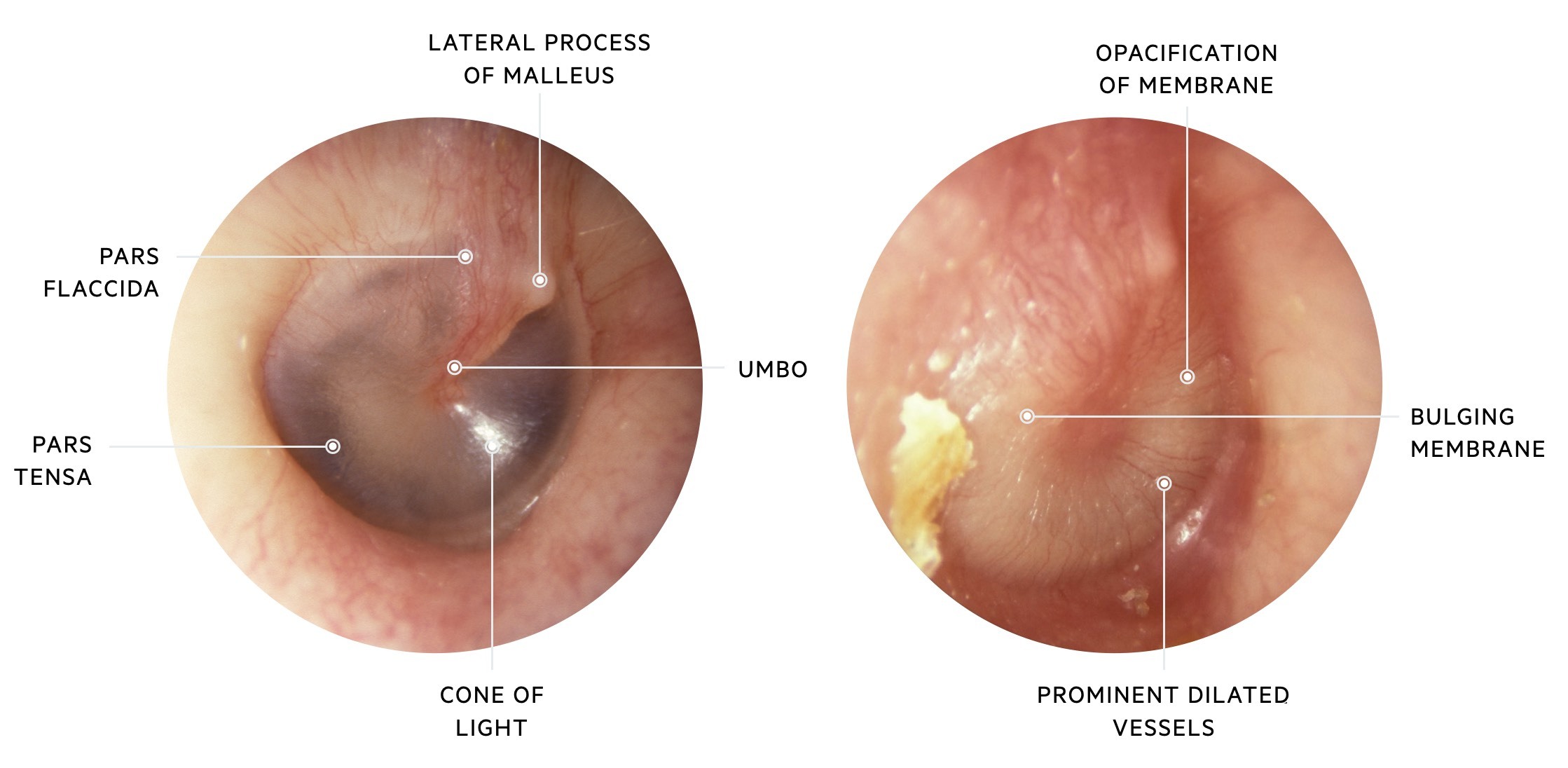
Otoscopy: Using an otoscope (lighted instrument), doctors examine the eardrum for:
- Redness and inflammation
- Bulging or retraction
- Fluid presence behind eardrum
- Reduced mobility
- Perforation or drainage
Pneumatic Otoscopy: Gentle air puffs test eardrum movement. Fluid-filled middle ears show reduced mobility.
Tympanometry: Device measures eardrum movement in response to air pressure changes, objectively assessing middle ear fluid and Eustachian tube function.
Acoustic Reflectometry: Measures sound reflected from eardrum, indicating fluid presence.
Hearing Tests: Audiometry assesses hearing loss severity, particularly important for chronic or recurrent infections potentially affecting speech and language development in children.
Tympanocentesis: Rarely performed procedure where needle aspirates middle ear fluid for bacterial culture in complicated or treatment-resistant cases.
According to the American Academy of Pediatrics, accurate diagnosis differentiating AOM from OME guides appropriate treatment decisions and prevents unnecessary antibiotic use.
Treatment Options: Effective Management Strategies
Watchful Waiting (Observation):
Not all otitis media requires immediate antibiotics. For children over 6 months with mild symptoms, doctors may recommend 48-72 hour observation with pain management, as many infections resolve spontaneously. This approach reduces antibiotic overuse and resistance.
Observation is appropriate when:
- Child over 6 months with non-severe symptoms
- Diagnosis uncertain
- Only one ear affected
- No fever or fever under 102.2°F (39°C)
- Pain manageable with over-the-counter medications
Pain Management:
Over-the-Counter Pain Relievers:
- Acetaminophen (Tylenol) for children over 2 months
- Ibuprofen (Advil, Motrin) for children over 6 months
- Dose according to weight and age guidelines
Topical Anesthetic Ear Drops: Provide temporary pain relief but don’t treat infection. Never use if eardrum perforation suspected.
Warm Compresses: Apply warm, damp cloth to affected ear for comfort.
Antibiotic Therapy:
When Antibiotics Are Necessary:
- Children under 6 months with confirmed AOM
- Severe symptoms (high fever, severe pain, bilateral infections)
- Symptoms persisting or worsening after 48-72 hours observation
- Complicated cases or high-risk patients
- Perforated eardrum with drainage
First-Line Antibiotics:
- Amoxicillin: Most commonly prescribed, effective against common bacteria
- Amoxicillin-clavulanate (Augmentin): For treatment failures or resistant bacteria
Alternative Antibiotics (penicillin allergies or resistance):
- Cephalosporins (cefdinir, cefuroxime)
- Azithromycin
- Clarithromycin
Treatment Duration: Typically 5-10 days, with shorter courses for older children and adults, longer for young children or complicated infections.
Important Antibiotic Principles:
- Complete entire prescribed course even if symptoms improve
- Never share antibiotics or use leftover prescriptions
- Follow up if symptoms don’t improve within 48-72 hours
Myringotomy and Ear Tubes:
For recurrent AOM or persistent OME causing hearing loss, surgical insertion of tympanostomy tubes (PE tubes) may be recommended. These tiny tubes:
- Equalize pressure across eardrum
- Allow fluid drainage
- Ventilate middle ear
- Dramatically reduce infection frequency
- Typically fall out naturally after 6-18 months
Adenoidectomy:
Removing enlarged adenoids blocking Eustachian tubes helps some children with recurrent infections or chronic effusion.
Managing Underlying Conditions:
Treating allergies, controlling environmental irritants, and addressing chronic sinusitis reduces otitis media risk, similar to comprehensive preventive care approaches.
Prevention Strategies: Reducing Infection Risk
Vaccination:
- Pneumococcal vaccine (PCV13): Significantly reduces S. pneumoniae infections
- Influenza vaccine: Annual flu shots reduce viral respiratory infections triggering otitis media
- Haemophilus influenzae type b (Hib) vaccine: Protects against another common bacterial cause
Breastfeeding:
Breastfeed exclusively for at least six months when possible. Breast milk provides antibodies and immune factors protecting against infections.
Feeding Position:
Hold babies upright (at least 30-45 degree angle) during bottle-feeding. Never prop bottles or allow babies to drink lying flat.
Pacifier Limitation:
Limit pacifier use after 6 months, particularly during sleep.
Smoke-Free Environment:
Never smoke around children. Eliminate all secondhand smoke exposure.
Hand Hygiene:

Frequent handwashing reduces respiratory infection transmission. Teach children proper hand hygiene practices.
Daycare Considerations:
Smaller daycare settings with fewer children reduce infection exposure. Ensure facilities follow strict illness policies and hygiene practices.
Allergy Management:
Control environmental and food allergies that contribute to Eustachian tube dysfunction.
Healthy Lifestyle:
Maintain balanced nutrition supporting immune function, ensure adequate sleep, and practice good overall health habits.
Complications: When to Worry
Most otitis media cases resolve without complications, but potential problems include:
Hearing Loss: Usually temporary from fluid, but chronic infections cause permanent damage.
Speech and Language Delays: Persistent hearing loss during critical developmental periods affects language acquisition in young children.
Tympanic Membrane Perforation: Eardrum tears from pressure, usually heals spontaneously but sometimes requires surgical repair.
Chronic Suppurative Otitis Media: Persistent infection with drainage requiring aggressive treatment.
Mastoiditis: Rare but serious infection spreading to mastoid bone behind ear, causing swelling, tenderness, fever, and requiring IV antibiotics or surgery.
Meningitis: Extremely rare complication where infection spreads to brain and spinal cord coverings, constituting medical emergency.
Brain Abscess: Very rare intracranial infection requiring emergency neurosurgical intervention.
Cholesteatoma: Abnormal skin growth in middle ear from chronic infections, requiring surgical removal.
Frequently Asked Questions About Otitis Media
Can ear infections spread from one person to another?
Otitis media itself isn’t contagious—you cannot “catch” an ear infection directly. However, the viruses and bacteria causing respiratory infections that lead to otitis media are highly contagious. When someone with a cold sneezes or coughs, others may contract the respiratory infection, potentially developing secondary ear infections if predisposed. Good hand hygiene and avoiding sick contacts reduce risk.
Why do some children get ear infections repeatedly?
Recurrent ear infections typically result from multiple factors including anatomical features (short, horizontal Eustachian tubes), immature immune systems, daycare attendance, smoke exposure, allergies, or genetic predisposition. Most children outgrow this tendency as Eustachian tubes mature and lengthen with growth, typically improving significantly after age 3-4. Until then, preventive measures and possibly ear tubes help manage recurrent infections.
Should my child stay home from school or daycare with an ear infection?
Children with otitis media aren’t contagious and can attend school or daycare once fever-free for 24 hours and feeling well enough to participate in activities. However, if the ear infection followed a viral respiratory infection, they may still be contagious from that underlying illness. Use judgment based on overall wellness, fever, and ability to function normally. Check with your facility’s illness policies.
Can adults get middle ear infections?
Yes, though far less commonly than children. Adult Eustachian tubes are longer, more vertical, and drain better, making infections less frequent. Adults developing otitis media often have underlying predisposing factors like chronic sinusitis, allergies, smoking, or anatomical abnormalities. Treatment principles are similar to children, though adults typically receive shorter antibiotic courses and rarely need ear tubes.
Will my child need ear tubes?
Most children never require ear tubes. Tubes are considered for recurrent acute otitis media (three episodes in six months or four in one year), chronic otitis media with effusion lasting three months or longer causing hearing loss, or when complications develop. Ear tubes are extremely safe, effective procedures performed as brief outpatient surgery. Your ENT specialist evaluates individual circumstances determining if tubes would benefit your child.
Navigating Middle Ear Infections Successfully
Middle ear infections, while common and often distressing, are highly manageable conditions with proper diagnosis and treatment. Understanding when antibiotics are necessary versus when watchful waiting is appropriate prevents antibiotic overuse while ensuring children receive appropriate care when needed. Effective pain management keeps children comfortable while infections resolve.
Prevention through vaccination, breastfeeding, smoke avoidance, and healthy practices significantly reduces infection frequency. For children with recurrent infections despite preventive measures, ear tubes provide excellent relief and dramatically improve quality of life.

Don’t hesitate to seek medical evaluation when children or adults develop ear pain, fever, or hearing changes. Early, appropriate treatment prevents complications and ensures optimal outcomes. Work collaboratively with healthcare providers, asking questions, expressing concerns, and participating in treatment decisions. Your advocacy ensures the best care for your child or yourself.
Remember that most children outgrow the tendency toward ear infections as they mature. Meanwhile, informed management, patience, and appropriate medical care help families navigate these challenging but temporary conditions successfully. With proper attention and care, middle ear infections remain manageable inconveniences rather than serious threats to health and development.
If you’re experiencing persistent ear symptoms or your child has recurrent infections, consult your healthcare provider or pediatric ENT specialist for comprehensive evaluation and personalized management strategies.

