Discover essential urinary incontinence treatments, recognize critical symptoms, and learn powerful prevention strategies. Comprehensive guide to regaining bladder control and confidence today.
Introduction
Urinary incontinence affects approximately 25 million Americans, causing involuntary bladder leakage that ranges from occasional minor drops to complete loss of bladder control. If you’ve experienced the embarrassment of unexpected leakage during a laugh, cough, or on the way to the bathroom, you’re far from alone. Despite its prevalence, many people suffer in silence due to shame or the mistaken belief that nothing can help. The truth? Urinary incontinence is highly treatable, and most people experience significant improvement with appropriate interventions.
This comprehensive guide reveals everything you need to know about urinary incontinence, from understanding different types to accessing powerful treatments that can restore your confidence and quality of life.
Understanding Urinary Incontinence: Beyond the Embarrassment
Urinary incontinence is the involuntary loss of urine—leaking when you don’t intend to. This isn’t merely an inconvenience or inevitable part of aging; it’s a medical condition with specific causes and effective treatments. The condition affects people of all ages, though it becomes more common with advancing age and affects women more frequently than men.
Normal bladder control involves complex coordination between your bladder muscle, sphincter muscles controlling urine release, pelvic floor muscles supporting bladder and urethra, and nerve signals communicating between bladder, spinal cord, and brain. Disruption at any point in this system can cause incontinence.
Types of Urinary Incontinence
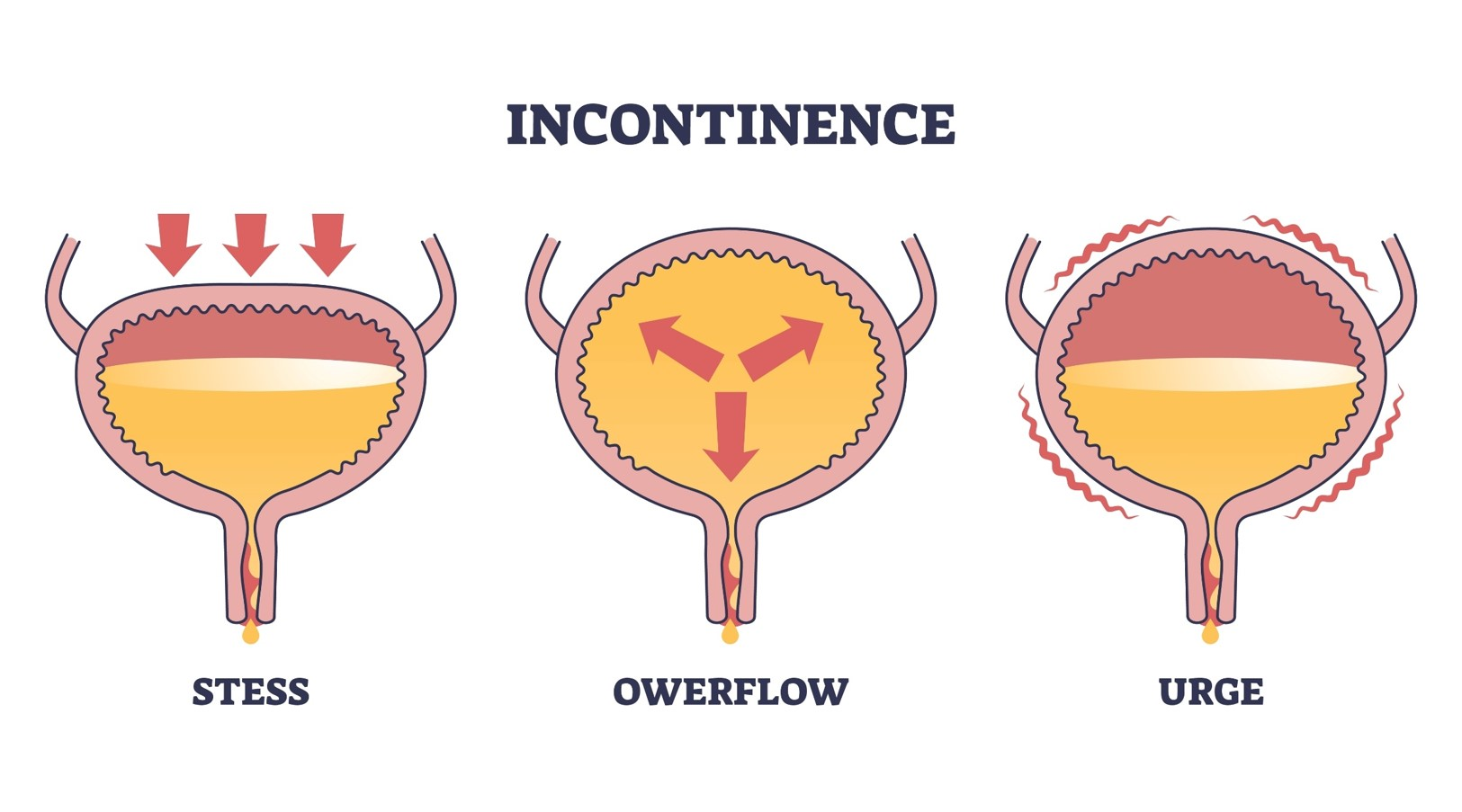
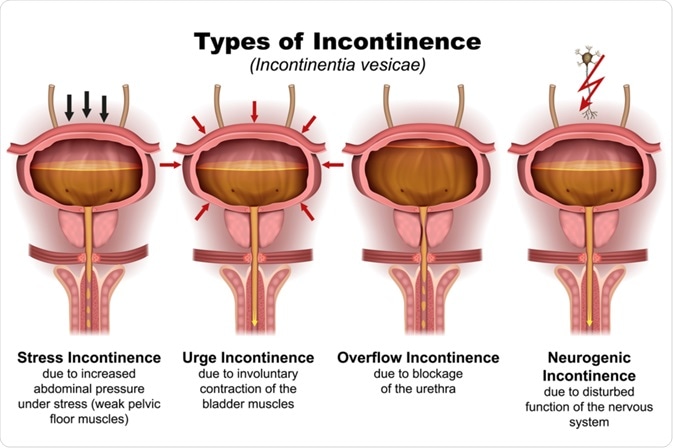
Stress incontinence, the most common type in younger women, involves urine leakage during activities that increase abdominal pressure—coughing, sneezing, laughing, exercising, or lifting heavy objects. This occurs when pelvic floor muscles and urethral sphincter weaken, failing to withstand sudden pressure increases.
Urge incontinence, also called overactive bladder, involves sudden, intense urges to urinate followed by involuntary bladder leakage. You may feel the need to urinate frequently—eight or more times in 24 hours—and wake multiple times nightly. This type results from overactive bladder muscles contracting involuntarily.
Mixed incontinence combines features of both stress and urge incontinence, affecting approximately one-third of incontinence sufferers. These individuals experience leakage both during physical activities and with sudden urges.
Overflow incontinence occurs when the bladder doesn’t empty completely, causing frequent or constant dribbling. This typically results from bladder muscle weakness or urethral blockage preventing normal emptying. It’s more common in men with prostate problems.
Functional incontinence happens when physical or mental impairments prevent reaching the bathroom in time despite normal bladder function. Conditions like severe arthritis limiting mobility or dementia affecting awareness exemplify causes.
Total incontinence involves continuous urine leakage due to complete sphincter dysfunction, anatomical abnormalities, or neurological conditions. This severe form is relatively uncommon.
Recognizing Risk Factors and Causes
Understanding what contributes to urinary incontinence helps target prevention and treatment strategies.
Gender-Specific Factors
Women experience incontinence more frequently than men due to pregnancy, childbirth, and menopause. Pregnancy hormones relax pelvic tissues, and the growing uterus increases bladder pressure. Vaginal delivery—particularly prolonged labor, large babies, or forceps delivery—can damage pelvic floor muscles, nerves, and supportive tissues.
Menopause brings declining estrogen levels that thin and weaken tissues lining the urethra and bladder, reducing support for continence mechanisms. These changes don’t guarantee incontinence but increase vulnerability.
Men primarily develop incontinence related to prostate problems. Enlarged prostate (benign prostatic hyperplasia) obstructs urine flow, causing overflow incontinence. Prostate cancer treatment—surgery or radiation—may damage nerves or sphincter muscles controlling continence.
Age and Lifestyle Factors
While not inevitable, aging brings changes increasing incontinence risk including decreased bladder capacity, reduced muscle strength and elasticity, and higher prevalence of chronic conditions affecting bladder function. However, many older adults maintain excellent continence, proving age alone doesn’t cause incontinence.
Obesity significantly increases incontinence risk by placing constant pressure on bladder and pelvic floor muscles. Even modest weight loss substantially improves or resolves incontinence in overweight individuals.
Smoking causes chronic coughing that strains pelvic floor muscles over time. Tobacco also irritates the bladder. Certain beverages and foods including caffeine, alcohol, carbonated drinks, artificial sweeteners, chocolate, spicy foods, and acidic foods can irritate the bladder and worsen symptoms.
Chronic constipation and straining during bowel movements weakens pelvic floor muscles shared between bladder and bowel control systems.
Medical Conditions
Neurological disorders including stroke, Parkinson’s disease, multiple sclerosis, or spinal cord injuries disrupt nerve signals controlling bladder function. Diabetes damages nerves throughout the body, including those controlling the bladder, and increases urine production.
Urinary tract infections cause temporary urgency and incontinence that typically resolve with antibiotic treatment. Certain medications including diuretics, sedatives, narcotics, antihistamines, and antidepressants may cause or worsen incontinence as side effects.
Comprehensive Diagnostic Approaches
Proper diagnosis identifies your specific incontinence type and underlying causes, guiding effective treatment.
Initial Evaluation
Your healthcare provider will conduct detailed medical history exploring symptom patterns, fluid intake, medications, previous surgeries, childbirth history, and medical conditions. Physical examination includes pelvic exam for women to assess muscle strength and identify anatomical issues, prostate exam for men, and neurological assessment checking reflexes and nerve function.
Bladder Diary
Keeping a detailed bladder diary for 3-7 days provides invaluable diagnostic information. Record times and amounts of urination, fluid intake, leakage episodes and circumstances, urgency sensations, and activities when leakage occurs. This log reveals patterns helping distinguish incontinence types and identify triggers.
Diagnostic Tests
Urinalysis checks for infection, blood, or other abnormalities. Post-void residual measurement uses ultrasound or catheterization to determine how much urine remains after urination—elevated residuals suggest incomplete emptying.
Urodynamic testing evaluates bladder function and pressure during filling and emptying. Cystoscopy allows direct bladder and urethra visualization through a thin, flexible scope, identifying structural abnormalities, stones, or tumors. These specialized tests help diagnose complex cases.
According to the National Association for Continence, proper diagnosis through comprehensive evaluation is essential for effective treatment, as different incontinence types require very different therapeutic approaches.
Powerful Treatment Options That Restore Control
Most people with urinary incontinence experience significant improvement through appropriate treatment. Starting with conservative approaches and progressing to more invasive options as needed maximizes success while minimizing risks.
Behavioral Therapies and Lifestyle Modifications
Bladder training gradually increases intervals between urination, teaching your bladder to hold more urine and reducing urgency. Start by urinating on schedule—every hour initially—rather than responding to every urge. Use distraction and relaxation techniques when urges occur between scheduled times. Gradually extend intervals by 15-30 minutes every week or two until reaching 3-4 hour intervals.
Scheduled toilet trips involve urinating on a fixed schedule—typically every 2-4 hours—preventing bladder from becoming too full. This approach works well for people with limited mobility or cognitive impairments.
Fluid management doesn’t mean restricting fluids excessively, which concentrates urine and irritates the bladder. Drink adequate amounts—typically 6-8 cups daily—but spread consumption throughout the day. Reduce evening intake to minimize nighttime urination. Identify and limit bladder irritants including caffeine, alcohol, carbonated beverages, and artificial sweeteners.
Maintain healthy weight management through balanced nutrition and regular physical activity. Research shows that losing just 5-10% of body weight significantly improves incontinence in overweight women.
Manage constipation through adequate fiber intake, proper hydration, and regular physical activity. Chronic constipation worsens incontinence by affecting pelvic floor function.
Pelvic Floor Muscle Training
Pelvic floor exercises, commonly called Kegel exercises, strengthen muscles supporting bladder control. These exercises benefit all incontinence types but prove particularly effective for stress and mixed incontinence.
To perform Kegels correctly, identify pelvic floor muscles by stopping urination midstream (do this only to locate muscles, not as regular practice). Tighten these muscles, hold for 3-5 seconds, then relax for 3-5 seconds. Gradually increase hold time to 10 seconds. Perform 10 repetitions, three times daily.
Avoid tightening abdominal, thigh, or buttock muscles during Kegels—focus solely on pelvic floor muscles. Breathe normally and don’t hold your breath. Consistency is crucial—like any exercise program, results require weeks to months of regular practice.
Physical therapists specializing in pelvic floor health can ensure proper technique, use biofeedback to help you isolate correct muscles, and develop personalized programs addressing your specific needs.
Medical Devices
Vaginal pessaries—small devices inserted into the vagina—support the bladder and urethra, reducing stress incontinence. Various shapes and sizes ensure proper fit. Healthcare providers fit pessaries and teach insertion, removal, and care.
Urethral inserts are small tampon-like disposable devices inserted before activities triggering leakage, removed before urination. These work for stress incontinence during specific activities like exercise.
Medications
For urge incontinence, anticholinergic medications including oxybutynin, tolterodine, and solifenacin block nerve signals causing involuntary bladder contractions. Beta-3 agonists like mirabegron relax bladder muscles through different mechanisms. These medications reduce urgency, frequency, and leakage episodes.
Topical estrogen for postmenopausal women helps restore urethral and vaginal tissue thickness and elasticity, improving symptoms related to hormonal changes. This local treatment avoids systemic hormone therapy risks.
Alpha-blockers help men with overflow incontinence from enlarged prostate by relaxing bladder neck and prostate muscles, improving urine flow.
Interventional Therapies
When conservative treatments prove insufficient, advanced options include:
Bulking agents injected around the urethra provide additional support, treating stress incontinence by adding bulk to tissues surrounding the urethra, helping it close more effectively.
Botulinum toxin (Botox) injections into the bladder muscle temporarily paralyze overactive areas, treating urge incontinence. Effects last 6-9 months, requiring repeat treatments.
Nerve stimulation therapies modulate signals between brain and bladder. Percutaneous tibial nerve stimulation (PTNS) involves weekly 30-minute sessions stimulating a nerve in the ankle. Sacral neuromodulation implants a device near the tailbone sending electrical pulses to bladder-controlling nerves.
Surgical Options
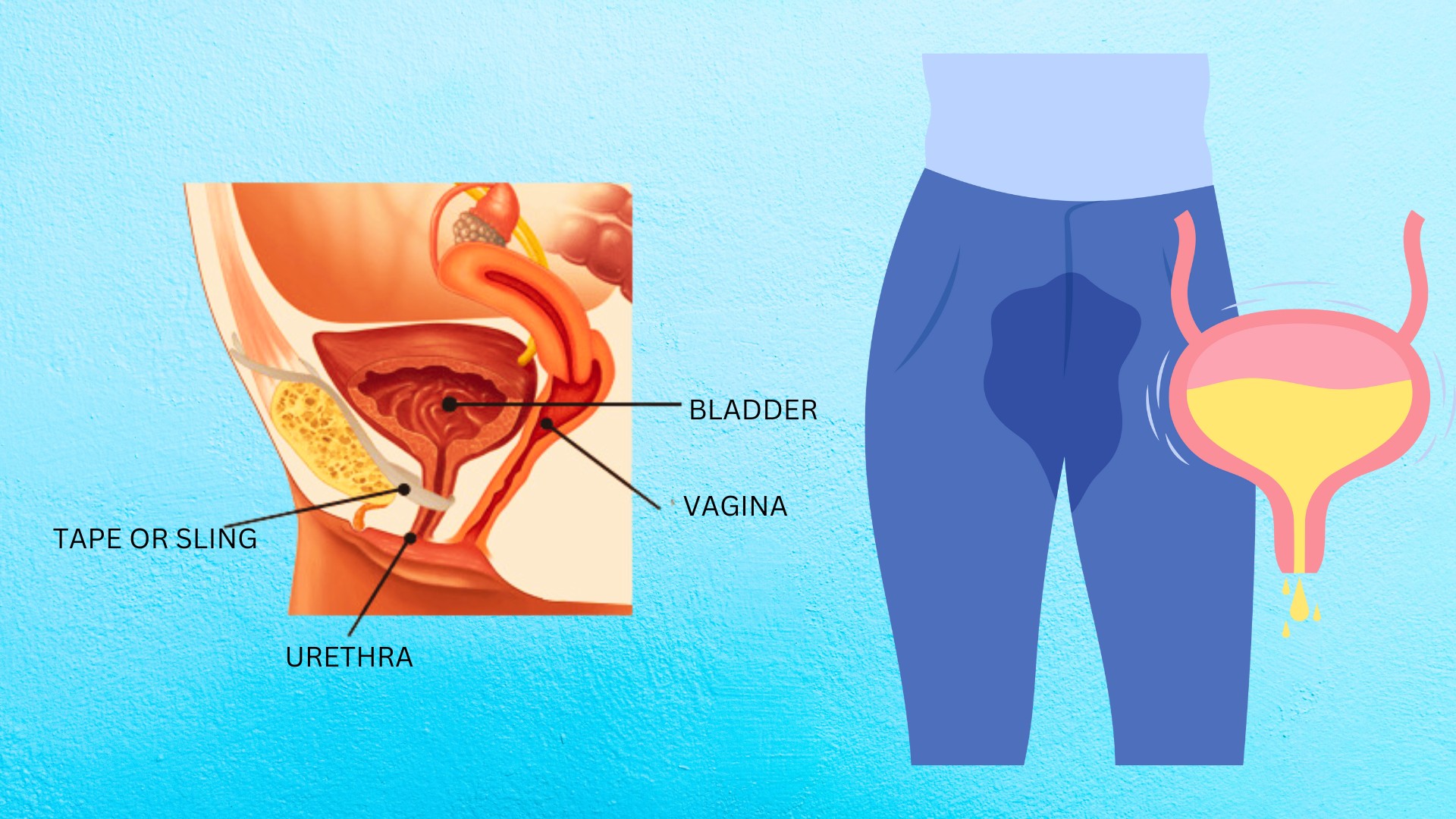
Various surgical procedures treat specific incontinence types when other treatments fail. Sling procedures create support under the urethra using synthetic mesh or tissue, treating stress incontinence. Bladder neck suspension lifts and supports the bladder neck and urethra. Artificial urinary sphincter implantation suits severe incontinence, particularly in men after prostate surgery.
Surgery carries risks and isn’t appropriate for everyone, but provides excellent results for properly selected candidates when conservative treatments fail.
Essential Self-Care and Daily Management
Successfully managing urinary incontinence extends beyond medical treatments to daily lifestyle practices.
Protective Products
While not treating underlying incontinence, absorbent products including pads, protective underwear, and adult diapers provide security and confidence managing unexpected leakage. Modern products are discreet, effective, and come in various absorbency levels. These should supplement, not replace, proper treatment.
Skin Care
Urine exposure irritates skin, causing rashes and breakdown. Keep skin clean and dry, gently cleanse after leakage episodes, apply barrier creams to protect skin, and change absorbent products promptly when soiled.
Clothing Choices
Wear clothing that’s easy to remove quickly—elastic waistbands, skirts, or pants with simple fasteners. Avoid complicated buttons, belts, or restrictive garments delaying bathroom access.
Bathroom Planning
When leaving home, identify bathroom locations in advance. Many smartphone apps locate public restrooms. Keep nightlights and clear pathways to bathrooms to prevent falls during nighttime trips.
Physical Activity
Regular exercise benefits incontinence by supporting weight management, strengthening core muscles, and improving overall health. Choose activities that don’t worsen symptoms—low-impact exercises like walking, swimming, or cycling are often well-tolerated. Empty your bladder before exercising. Consider using absorbent protection during workout routines if needed for confidence.
Emotional Wellbeing
Living with incontinence affects mental wellness. Anxiety, embarrassment, and social isolation are common. Recognize these feelings as normal but treatable. Professional counseling, support groups, and sometimes medication help manage emotional aspects. Don’t let incontinence prevent you from enjoying meaningful activities and relationships.
Prevention Strategies That Work
While not all incontinence is preventable, certain practices reduce risk and support bladder health.
Maintain Pelvic Floor Strength
Practice pelvic floor exercises throughout life, particularly during and after pregnancy. These exercises benefit prevention even if you’ve never experienced incontinence. Men also benefit from pelvic floor training, particularly before and after prostate surgery.
Healthy Lifestyle Habits
Maintain healthy weight through balanced diet and regular physical activity. Avoid smoking and excessive alcohol consumption. Treat chronic coughs promptly rather than allowing them to persist and strain pelvic muscles. Address constipation through adequate fiber, fluids, and physical activity.
Practice Good Voiding Habits
Don’t delay urination excessively when feeling the urge—chronic overfilling may weaken bladder muscles. Conversely, avoid “just in case” urination when you don’t actually need to go, as this trains the bladder to signal urgency at small volumes. Take adequate time to empty completely without straining.
Manage Chronic Conditions
Control diabetes through proper medication, diet, and lifestyle. Treat urinary tract infections promptly. Address neurological conditions with appropriate medical care. These proactive approaches support overall bladder health.
Frequently Asked Questions About Urinary Incontinence
Is urinary incontinence a normal part of aging?
No, while incontinence becomes more common with age, it’s not an inevitable part of aging. Many older adults maintain excellent bladder control throughout their lives. Incontinence is a medical condition with specific causes requiring treatment. Don’t dismiss symptoms as “just getting older”—effective treatments exist that can dramatically improve quality of life regardless of age.
Will Kegel exercises really help?
Yes, pelvic floor exercises effectively treat stress and mixed incontinence when performed correctly and consistently. Research shows that 60-70% of women with stress incontinence improve significantly with proper pelvic floor training. The key is correct technique, adequate intensity, and consistency over several months. Working with a pelvic floor physical therapist ensures proper form and maximizes results.
Can men get urinary incontinence?
Yes, though less common than in women, men develop urinary incontinence, particularly related to prostate problems. Enlarged prostate causes overflow incontinence, while prostate cancer treatment may cause stress incontinence. Men benefit from pelvic floor exercises, lifestyle modifications, and medical treatments similar to women, though specific interventions may differ based on underlying causes.
Will I need surgery?
Most people with urinary incontinence never require surgery. Conservative treatments including lifestyle modifications, pelvic floor exercises, and medications effectively manage symptoms for the majority of patients. Surgery is typically considered only when conservative treatments fail or for specific anatomical abnormalities. Many people achieve excellent results without ever needing surgical intervention.
How long does treatment take to work?
Timeline varies by treatment type. Lifestyle modifications may show initial improvements within weeks. Pelvic floor exercises typically require 6-12 weeks of consistent practice for significant improvement. Medications may help within days to weeks. Surgical procedures often provide immediate improvement. Patience and persistence are crucial—don’t abandon effective treatments prematurely.
Can urinary incontinence be cured?
Many cases of urinary incontinence can be cured or improved to the point where symptoms no longer significantly impact daily life. Success depends on incontinence type, underlying causes, and treatment adherence. Stress incontinence often resolves completely with pelvic floor training or surgery. Urge incontinence typically improves dramatically with appropriate treatment, though ongoing management may be needed.
Should I limit fluids to reduce leakage?
No, excessive fluid restriction is harmful. Dehydration concentrates urine, which irritates the bladder and may worsen symptoms. It also causes other health problems. Drink adequate fluids—typically 6-8 cups daily—but spread consumption throughout the day. Reduce evening intake to minimize nighttime urination. The goal is adequate hydration without excess, not restriction.
Will wearing pads make my bladder weaker?
No, using absorbent products doesn’t weaken your bladder or pelvic floor muscles. These products provide security and confidence while you pursue proper treatment. However, pads and protective underwear should supplement, not replace, addressing underlying causes. Don’t rely solely on protective products—seek treatment for the incontinence itself while using products as needed for security.

