Discover critical ulcer warning signs, powerful treatment options, and essential prevention strategies. Comprehensive guide to healing peptic ulcers and reclaiming your digestive health today.
Introduction
Peptic ulcers affect approximately 4.5 million Americans annually, causing burning abdominal pain that can range from mildly uncomfortable to absolutely debilitating. If you’ve experienced gnawing stomach pain, especially between meals or at night, you understand how significantly ulcers impact quality of life. The encouraging news? Modern medicine has revolutionized ulcer treatment, transforming what was once a chronic, recurring condition into one that’s highly curable with proper care.
This comprehensive guide reveals everything you need to know about ulcers, from recognizing warning signs to accessing powerful treatments that can heal your digestive system and prevent recurrence.
Understanding Peptic Ulcers: More Than Just Stomach Pain
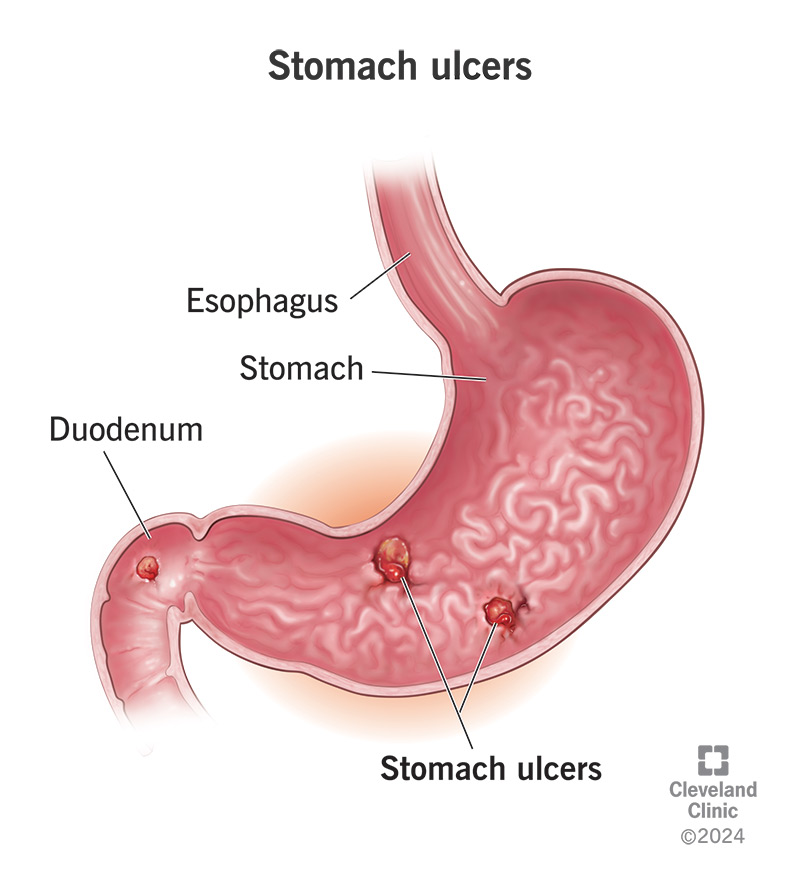
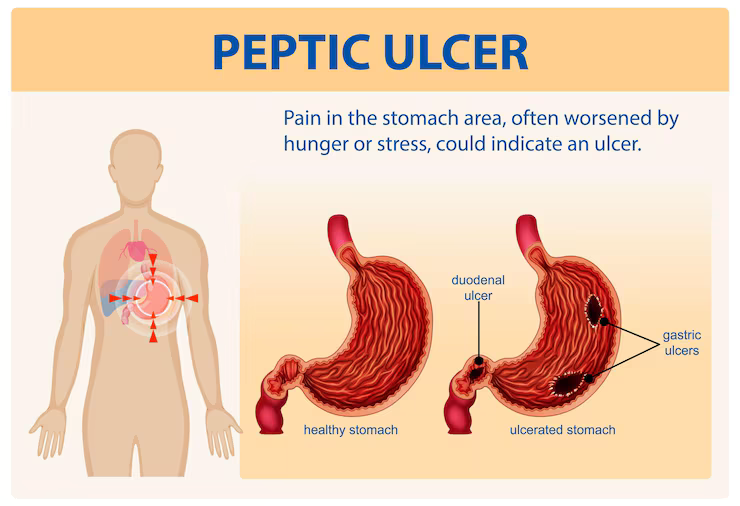
Peptic ulcers are open sores that develop on the inner lining of your stomach, upper small intestine (duodenum), or occasionally the esophagus. These painful lesions occur when the protective mucus layer lining your digestive tract breaks down, allowing stomach acid to damage underlying tissues.
Your stomach produces hydrochloric acid strong enough to digest food and kill bacteria. Normally, a thick mucus layer protects stomach and intestinal walls from this corrosive acid. When this protective barrier becomes compromised, acid erodes the delicate lining, creating ulcers.
Types of Peptic Ulcers
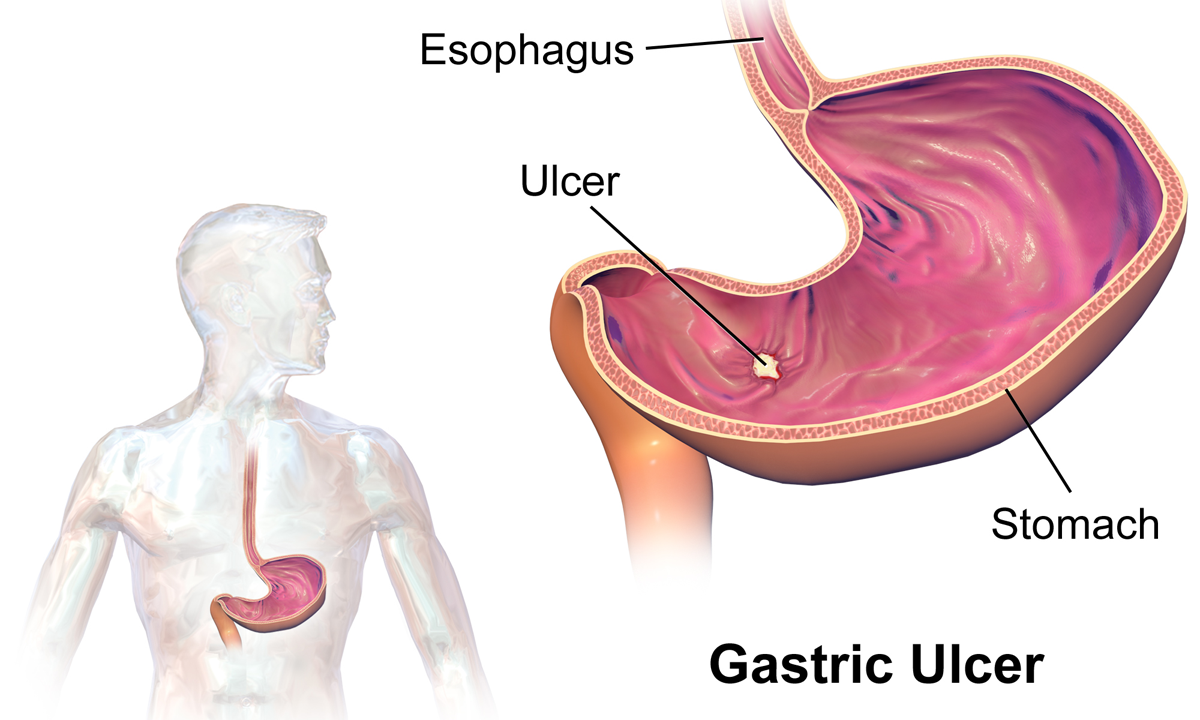
Gastric ulcers develop in the stomach lining and typically cause pain during or shortly after eating, as food and acid contact the sensitive ulcer. People with gastric ulcers often experience reduced appetite and may lose weight due to pain associated with eating.
Duodenal ulcers form in the first part of the small intestine (duodenum) and represent the most common ulcer type, accounting for about 80% of cases. These typically cause pain 2-3 hours after eating or during the night when the stomach is empty. Eating or taking antacids often provides temporary relief.
Esophageal ulcers, though less common, develop in the lower esophagus, usually related to chronic acid reflux (GERD). These cause painful swallowing and chest discomfort.
The Revolutionary Discovery: H. Pylori and Ulcers
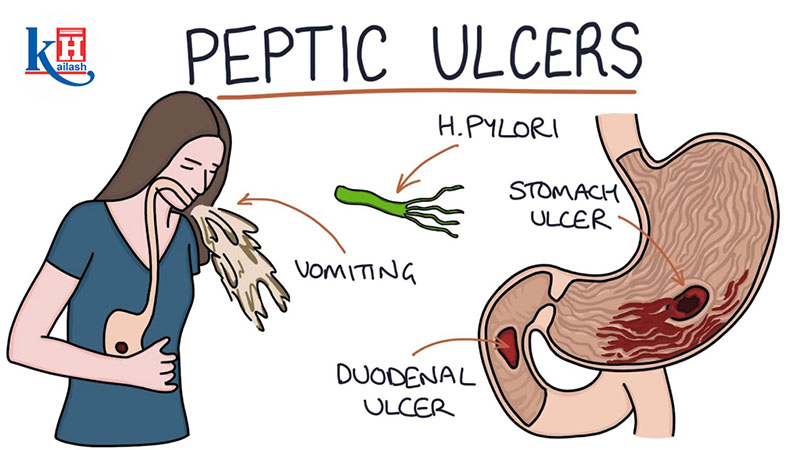
For decades, doctors believed stress and spicy foods caused ulcers, recommending bland diets and stress reduction. This changed dramatically in the 1980s when Australian researchers Barry Marshall and Robin Warren discovered that a bacterium called Helicobacter pylori (H. pylori) causes most ulcers—a finding that earned them the 2005 Nobel Prize in Medicine.
How H. Pylori Causes Ulcers
H. pylori is a spiral-shaped bacterium uniquely adapted to survive in the stomach’s harsh acidic environment. It burrows into the protective mucus layer and produces enzymes that neutralize surrounding stomach acid, creating a safe microenvironment.
The bacterium then damages the mucus layer and underlying cells through multiple mechanisms, triggering inflammation and reducing protective mucus production. This compromised barrier allows stomach acid to erode the lining, forming ulcers. H. pylori infects approximately 50% of the global population, though most infected people never develop ulcers.
According to the American College of Gastroenterology, H. pylori causes approximately 60% of gastric ulcers and 90% of duodenal ulcers, making bacterial eradication crucial for successful treatment and preventing recurrence.
The NSAID Connection
The second major ulcer cause is regular use of nonsteroidal anti-inflammatory drugs (NSAIDs) including aspirin, ibuprofen, naproxen, and prescription NSAIDs. These medications inhibit enzymes that protect the stomach lining while reducing inflammation and pain throughout the body.
Regular NSAID use—particularly at high doses or for extended periods—significantly increases ulcer risk. Combining NSAIDs with other risk factors like H. pylori infection, alcohol use, or corticosteroids dramatically elevates ulcer development probability.
Recognizing Critical Warning Signs
Understanding ulcer symptoms enables early detection and treatment, preventing serious complications.
Primary Symptoms
Burning stomach pain represents the hallmark symptom, typically described as gnawing, aching, or burning sensation in the upper abdomen between the breastbone and navel. This pain follows characteristic patterns: duodenal ulcer pain often occurs 2-3 hours after meals and may awaken you at night, improving with eating or antacids. Gastric ulcer pain typically worsens during or shortly after meals.
Pain intensity varies from mild discomfort to severe, debilitating pain. Some people experience constant pain while others have intermittent symptoms with pain-free periods.
Associated Symptoms
Nausea and vomiting sometimes accompany ulcer pain, particularly with gastric ulcers. Bloating and feeling full quickly after eating small amounts suggests ulcers. Loss of appetite and unintentional weight loss may occur, especially with gastric ulcers where eating triggers pain. Heartburn and acid reflux symptoms often coexist with ulcers.
Dangerous Complications Requiring Emergency Care
Certain symptoms indicate serious complications demanding immediate medical attention. Vomiting blood—appearing bright red or resembling coffee grounds—signals bleeding ulcers. Black, tarry, or bloody stools indicate gastrointestinal bleeding. Severe, sudden, intense abdominal pain may indicate perforation where the ulcer creates a hole through the stomach or intestinal wall.
Persistent vomiting preventing fluid retention causes dehydration and electrolyte imbalances. Unexplained significant weight loss warrants evaluation. These complications, though uncommon with modern treatment, can be life-threatening without prompt care.
Comprehensive Diagnostic Approaches
Accurate diagnosis ensures appropriate treatment targeting underlying causes.
Initial Evaluation
Your healthcare provider will conduct detailed medical history exploring symptom patterns, NSAID use, previous ulcers, family history, and smoking or alcohol consumption. Physical examination includes abdominal palpation checking for tenderness, masses, or other abnormalities.
H. Pylori Testing
Several tests detect H. pylori infection. Breath tests involve drinking a special solution then providing breath samples. H. pylori produces enzymes breaking down the solution, releasing detectable gases. Stool antigen tests identify H. pylori proteins in stool samples. Blood antibody tests detect immune system response to H. pylori, though they can’t distinguish current from past infections.
Biopsy during endoscopy provides definitive H. pylori diagnosis through tissue samples tested for bacterial presence.
Endoscopy
Upper endoscopy (esophagogastroduodenoscopy or EGD) involves inserting a thin, flexible tube with a camera through your mouth into the esophagus, stomach, and duodenum. This allows direct visualization of ulcers, assessment of their size and location, and collection of tissue samples (biopsies) for H. pylori testing and cancer screening.
Endoscopy is recommended for people with alarm symptoms (bleeding, weight loss, difficulty swallowing), those over 60 with new symptoms, and when diagnosis is uncertain.
Imaging Studies
Upper gastrointestinal (GI) series uses X-rays after drinking barium solution that coats your digestive tract, making ulcers visible on X-rays. This less invasive test helps when endoscopy isn’t feasible, though it provides less detailed information than endoscopy.
Powerful Treatment Strategies That Heal
Modern ulcer treatment achieves healing rates exceeding 90% when patients complete full treatment courses.
H. Pylori Eradication Therapy
If H. pylori is detected, eradication requires combination therapy called “triple therapy” or “quadruple therapy.” Triple therapy typically includes a proton pump inhibitor (PPI) reducing stomach acid, plus two antibiotics like clarithromycin and amoxicillin (or metronidazole for penicillin-allergic patients), taken for 10-14 days.
Quadruple therapy adds bismuth subsalicylate to a PPI and two different antibiotics, used when triple therapy fails or in areas with high antibiotic resistance.
Completing the entire antibiotic course is crucial even if symptoms improve quickly. Incomplete treatment allows H. pylori to persist and develop antibiotic resistance. Follow-up testing 4-6 weeks after completing treatment confirms eradication.
Acid-Suppressing Medications
Proton pump inhibitors (PPIs) like omeprazole, lansoprazole, esomeprazole, and pantoprazole powerfully suppress acid production, allowing ulcers to heal. For H. pylori-negative ulcers or those caused by NSAIDs, PPIs are typically continued for 4-8 weeks.
H2 receptor antagonists including famotidine, ranitidine, and cimetidine also reduce acid production, though less potently than PPIs. These may suffice for milder ulcers or serve as step-down therapy after initial PPI treatment.
Antacids provide rapid but temporary symptom relief by neutralizing existing stomach acid. They don’t heal ulcers but help manage discomfort between medication doses.
NSAID Management
If NSAIDs caused your ulcer, discontinuing them is crucial when possible. Discuss alternatives with your healthcare provider—acetaminophen may substitute for pain relief without ulcer risk.
If NSAID use must continue for conditions like arthritis or cardiovascular protection, strategies to reduce ulcer risk include using the lowest effective dose, taking NSAIDs with food, combining NSAIDs with PPIs for protection, or switching to selective COX-2 inhibitors that carry lower (though not absent) ulcer risk.
Lifestyle Modifications
While lifestyle changes don’t cure ulcers alone, they support healing and prevent recurrence. Avoid foods and beverages that worsen symptoms—common triggers include alcohol, caffeine, chocolate, spicy foods, and acidic foods like citrus and tomatoes. Individual tolerance varies, so identify your personal triggers.
Quit smoking, as tobacco increases ulcer risk, impairs healing, and promotes recurrence. Smoking stimulates acid production and reduces blood flow to the stomach lining, interfering with protective mechanisms.
Manage stress and anxiety, which don’t cause ulcers but may worsen symptoms and slow healing. Practice stress-reduction techniques including meditation, deep breathing, regular exercise, and adequate sleep.
Maintain balanced nutrition supporting overall health and healing. While no specific diet treats ulcers, adequate protein, vitamins, and minerals support tissue repair. Eating smaller, more frequent meals may reduce symptom severity for some people.
Prevention: Keeping Ulcers From Returning
Once your ulcer heals, prevention focuses on addressing underlying causes and risk factors.
Successful H. Pylori Eradication
Confirming H. pylori elimination through follow-up testing is crucial. If the bacterium persists, repeat treatment with different antibiotic combinations prevents recurrence. Successfully eradicating H. pylori dramatically reduces ulcer recurrence rates.
Reinfection is uncommon in developed countries with good sanitation. H. pylori spreads through contaminated food, water, or close contact with infected individuals. Good hygiene practices including handwashing reduce transmission risk.
Safe Pain Medication Use
If you need regular pain relief, explore NSAID alternatives when possible. Acetaminophen provides effective pain relief for many conditions without ulcer risk. For conditions requiring NSAIDs, use the lowest effective dose for the shortest duration necessary.
Take NSAIDs with food to minimize stomach irritation. Your doctor may prescribe protective medications (PPIs or misoprostol) if you require ongoing NSAID therapy, particularly if you have ulcer history or other risk factors.
Lifestyle Factors
Limit alcohol consumption, as excessive intake damages the stomach lining and increases acid production. Moderate consumption (up to one drink daily for women, two for men) is generally safe, though individual tolerance varies.
Maintain healthy weight management and overall wellness through balanced diet and regular physical activity. While obesity doesn’t directly cause ulcers, maintaining healthy weight reduces numerous health risks and supports digestive health.
Practice stress management through regular exercise routines, adequate sleep, and relaxation techniques. While stress doesn’t cause ulcers, chronic stress affects overall health and may influence digestive function.
Natural Approaches and Complementary Therapies
While these shouldn’t replace medical treatment, certain natural approaches may support ulcer healing alongside conventional therapy.
Dietary Considerations
Foods with potential ulcer-healing properties include probiotics from yogurt, kefir, and fermented foods that may help combat H. pylori and support gut health. Honey, particularly Manuka honey, possesses antibacterial properties and may help inhibit H. pylori growth. Cruciferous vegetables like broccoli contain sulforaphane, which may fight H. pylori.
Flavonoid-rich foods including apples, berries, celery, and tea have antioxidant and anti-inflammatory properties potentially supporting healing. However, scientific evidence supporting specific foods for ulcer treatment remains limited.
Herbal Remedies
Some herbs show promise in preliminary studies. Licorice root (deglycyrrhizinated licorice or DGL) may protect stomach lining. Mastic gum may have antibacterial effects against H. pylori. Slippery elm might coat and soothe the digestive tract.
Always discuss herbal supplements with your healthcare provider before use, as they can interact with medications and aren’t substitutes for proven medical treatments.
Special Considerations and Populations
Older Adults
Ulcer risk increases with age due to higher NSAID use for arthritis and other conditions, increased H. pylori infection prevalence, and age-related changes in stomach lining and acid production. Older adults may experience less obvious symptoms, delaying diagnosis. Regular monitoring when using NSAIDs and prompt evaluation of digestive symptoms are crucial.
People With Chronic Conditions
Certain conditions increase ulcer risk. Those requiring daily aspirin for cardiovascular protection need careful monitoring and often prophylactic PPIs. People with rheumatoid arthritis or other conditions requiring regular NSAIDs benefit from protective strategies. Chronic kidney disease, liver disease, and other serious illnesses may complicate ulcer treatment.
During Pregnancy
Pregnancy presents unique challenges as some ulcer medications aren’t recommended during pregnancy or breastfeeding. Discuss all medications with your obstetrician. Lifestyle modifications and safe medications like certain antacids may manage symptoms during pregnancy.
Long-Term Outlook and Living Well
With appropriate treatment, most ulcers heal completely within 4-8 weeks, and recurrence rates drop dramatically when underlying causes are addressed. Successfully eradicating H. pylori reduces recurrence risk to less than 5%, compared to 50-90% recurrence rates when the infection persists.
Most people return to normal activities and eating patterns after healing. While some dietary modifications during acute ulcer phases may help, restrictive long-term diets aren’t necessary once healed. Focus on overall balanced healthy eating rather than unnecessary restrictions.
Regular medical follow-up ensures complete healing and addresses any complications. Maintain open communication with your healthcare team about persistent or recurrent symptoms.
Frequently Asked Questions About Ulcers
Can stress cause ulcers?
No, stress doesn’t directly cause ulcers. This common misconception persisted for decades until H. pylori bacteria and NSAID use were identified as primary causes. However, stress may worsen existing ulcer symptoms and potentially slow healing. Managing stress supports overall health and may improve symptom management, but stress reduction alone won’t cure ulcers caused by H. pylori or NSAIDs.
Do spicy foods cause ulcers?
No, spicy foods don’t cause ulcers, though they may irritate existing ulcers and worsen symptoms in some people. Once your ulcer heals, most people can resume eating spicy foods without problems. Individual tolerance varies—if certain foods trigger symptoms, avoid them, but dietary restrictions aren’t necessary for everyone with ulcer history.
How long does it take for ulcers to heal?
With appropriate treatment, most uncomplicated ulcers heal within 4-8 weeks. Larger ulcers may require longer treatment periods. H. pylori eradication combined with acid suppression achieves healing rates exceeding 90%. Following your complete treatment regimen and attending follow-up appointments ensures proper healing. Symptoms often improve within days to weeks, though complete healing takes longer.
Can ulcers turn into cancer?
Peptic ulcers themselves don’t become cancerous. However, chronic H. pylori infection increases stomach cancer risk independently of ulcers. This is one reason H. pylori eradication is crucial. Additionally, what appears to be an ulcer on endoscopy occasionally turns out to be stomach cancer, which is why biopsies are taken during endoscopy, particularly in people over 60 or with alarm symptoms.
Will my ulcer come back?
Recurrence risk depends on addressing underlying causes. Successfully eradicating H. pylori reduces recurrence to less than 5%. Continuing NSAIDs without protective measures carries high recurrence risk. Smoking increases recurrence likelihood. Following prevention strategies dramatically reduces the chance of developing future ulcers.
Can I drink coffee with an ulcer?
Coffee and caffeine stimulate acid production and may irritate ulcers, potentially worsening symptoms. During active ulcer healing, limiting or avoiding coffee and other caffeinated beverages may help. Once healed, many people can resume moderate coffee consumption. Pay attention to your body—if coffee triggers symptoms, reduce or eliminate it. Decaffeinated coffee also stimulates acid production, though less than regular coffee.
Are there complications from long-term PPI use?
Long-term PPI use (years of continuous therapy) has been associated with potential risks including decreased calcium absorption increasing fracture risk, vitamin B12 deficiency, increased infection susceptibility, and rarely, kidney problems. However, for most people requiring PPIs, benefits outweigh risks. Use the lowest effective dose for the necessary duration. Discuss long-term PPI use with your healthcare provider to balance benefits and risks.
How is H. pylori transmitted?
H. pylori spreads through oral-fecal and oral-oral routes, typically during childhood. Contaminated food or water, close contact with infected individuals (particularly within families), and poor sanitation contribute to transmission. In developed countries with good sanitation, transmission is less common. Good hygiene practices including thorough handwashing reduce transmission risk, though casual contact doesn’t typically spread H. pylori.

