Comprehensive guide to prostate cancer stages and treatment options. Learn about TNM staging, Grade Groups, surgery vs radiation, active surveillance, and personalized treatment strategies for localized and advanced prostate cancer.
Introduction
Every three minutes, an American man receives a prostate cancer diagnosis—a life-altering moment that immediately raises critical questions about survival, treatment, and quality of life. Prostate cancer represents the most common non-skin cancer affecting men, yet outcomes vary dramatically depending on when it’s detected and how it’s staged. Understanding the staging system empowers patients to have meaningful conversations with their healthcare team, evaluate treatment options, and make informed decisions that align with their priorities and values.
The good news? Most men with prostate cancer live long, productive lives after diagnosis. Although prostate cancer is the most common cancer in men in the United States, it comes with a relatively good prognosis, with most men with prostate cancer still alive 15 years after their diagnosis. This encouraging statistic underscores the importance of accurate staging and appropriate treatment selection—decisions that profoundly impact both survival and quality of life.
Decoding the TNM Staging System
The most widely used staging system for prostate cancer is the AJCC (American Joint Committee on Cancer) TNM system, which was most recently updated in 2018. This standardized framework enables physicians worldwide to communicate precisely about cancer extent and guide treatment recommendations.
The Three Pillars of TNM Classification
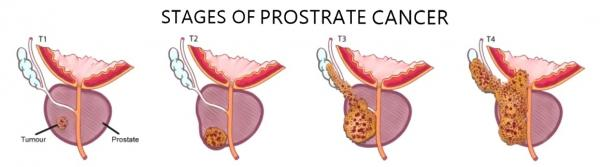
T – Tumor Extent: This describes how far cancer has grown within or beyond the prostate gland. There are 4 main T stages of prostate cancer – T1 to T4, with T1 meaning the cancer is too small to be seen on a scan or felt during an examination of the prostate. The T category progresses from T1 (cancer detected through biopsy after elevated PSA) through T2 (cancer confined within the prostate) to T3 (cancer extending beyond the prostate capsule) and T4 (cancer invading nearby structures like the bladder or rectum).
Understanding the distinction between clinical and pathological T staging matters tremendously. The clinical T category (cT) is your doctor’s best estimate based on physical exam and imaging, while the pathological T category (pT) is determined by examining the entire prostate in the lab after surgery, making it likely to be more accurate.
N – Nodal Involvement: This indicates whether cancer has spread to nearby lymph nodes. N1 means there are cancer cells in lymph nodes near the prostate, while N0 indicates no nodal involvement. Lymph node status significantly affects prognosis and treatment decisions, particularly regarding the need for systemic therapies.
M – Metastasis: This reveals whether cancer has spread to distant sites. M0 means the cancer hasn’t spread to other parts of your body, while M1 means the cancer has spread to other parts of the body outside the pelvis, split into M1a (lymph nodes outside the pelvis), M1b (bones), and M1c (other organs).
The Critical Role of Grade Groups
The Grade Group (based on the Gleason score) is a measure of how likely the cancer is to grow and spread quickly, determined by results of the prostate biopsy or surgery. This grading system examines cancer cell appearance under microscopy, with Grade Group 1 representing the most well-differentiated (least aggressive) cells and Grade Group 5 indicating poorly differentiated (most aggressive) cells.
The Gleason score combines patterns of two most common cancer cell appearances, resulting in scores ranging from 6 (3+3) to 10 (5+5). Modern staging incorporates Grade Groups because two cancers with identical T, N, and M classifications but different grades behave very differently, requiring distinct treatment approaches.
PSA Levels Complete the Picture
Prostate-specific antigen (PSA) blood levels provide additional prognostic information. When T, N, and M categories have been determined, this information is combined along with the Grade Group and PSA level if available in a process called stage grouping to get the overall stage of the cancer. This integrated approach creates a comprehensive risk assessment that guides treatment selection.
Understanding Stage Groupings: From I to IV
Combining TNM classification, Grade Groups, and PSA levels produces overall stages ranging from Stage I through Stage IV, each with distinct implications for treatment and prognosis.
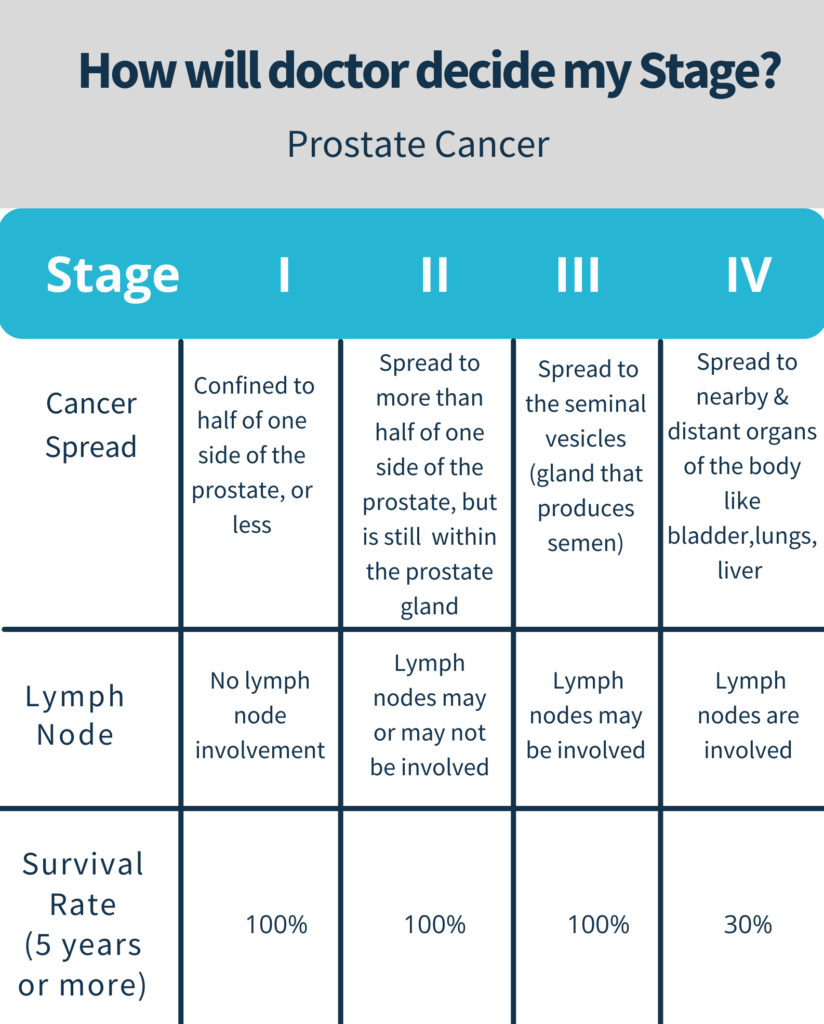
Stage I: The Most Favorable Outlook
The prostate cancer cannot be felt during a digital rectal exam and cannot be seen on a sonogram, often found during surgery for another non-cancerous reason, usually for benign prostatic hyperplasia, with cancer only in the prostate and the grade being G1 or the Gleason score no higher than 4. Men diagnosed at Stage I typically have excellent long-term survival prospects and may be candidates for active surveillance rather than immediate treatment.
Stage II: Confined But More Concerning
Stage II subdivides into IIA, IIB, and IIC based on tumor size, PSA levels, and cell differentiation. Stage IIA involves a tumor that cannot be felt and involves half of one side of the prostate or even less, with PSA levels being medium and cancer cells well differentiated, while Stage IIB and IIC involve progressively higher-grade tumors or larger sizes. Stage II cancers remain confined within the prostate but show characteristics suggesting more aggressive behavior requiring definitive treatment.
Stage III: Locally Advanced Disease
The tumor has grown outside of the prostate and may have invaded the seminal vesicles but has not spread to the lymph nodes, with Stage IIIA involving cancer that has spread beyond the outer layer of the prostate into nearby tissues or seminal vesicles. Stage IIIC indicates cancer cells across the tumor are poorly differentiated, meaning they look very different from healthy cells. Stage III disease typically requires multimodal therapy combining local treatment with systemic approaches.
Stage IV: Metastatic Cancer
Stage IVA means the cancer has spread to the regional lymph nodes, while Stage IVB indicates the cancer has spread to distant lymph nodes, other parts of the body, or to the bones. Stage IV prostate cancer requires systemic therapies focusing on controlling disease progression, managing symptoms, and maximizing quality of life rather than curative local treatments alone.
Risk Stratification: Refining Treatment Decisions
Beyond basic staging, physicians use risk stratification systems to further personalize treatment recommendations. Doctors group prostate cancer into risk groups, with the UK now using the Cambridge Prognostic Group (CPG) system that divides prostate cancer into 5 risk groups, combining Grade Group, PSA and T stage.
The EAU risk group classification, essentially based on D’Amico’s classification system for prostate cancer, combines clinical information on tumor extent, PSA and pathology from systematic biopsy. These risk groups—typically categorized as low, intermediate, and high—help distinguish patients who may safely defer treatment from those requiring aggressive intervention.
Understanding your risk group matters because it directly influences whether active surveillance, surgery, radiation, or combination therapies represent the most appropriate strategy. Two men with the same T stage might receive entirely different treatment recommendations based on their Grade Group and PSA levels.
Treatment Options for Localized Prostate Cancer
When cancer remains confined to the prostate, patients typically face decisions among active surveillance, surgery, and radiation therapy. According to the American Cancer Society, all treatment options—surgery, external radiation, and internal radiation—are similarly effective for early stage prostate cancer, with treatment choices often depending on a person’s overall health and preference.
Active Surveillance: Watching and Waiting Wisely
For carefully selected low-risk patients, active surveillance represents a valid approach. This strategy involves regular monitoring through PSA testing, digital rectal exams, and periodic biopsies, only initiating treatment if cancer shows signs of progression. Men with cancer confined to the prostate and at low risk experienced different long-term side effects depending on the type of treatment received, making understanding the pros and cons of different treatments important for informed treatment decisions.
Active surveillance avoids treatment-related side effects while cancer remains indolent, preserving quality of life without compromising long-term survival for appropriately selected patients. However, it requires psychological comfort with “living with cancer” and commitment to rigorous monitoring protocols.
Radical Prostatectomy: Surgical Removal
Surgery involves complete prostate gland removal along with surrounding tissue. A radical prostatectomy involves cutting the tube that connects the testes, which make sperm, to the urethra, meaning a person who undergoes this surgery can no longer conceive a child through typical methods, though there are options for fertility preservation such as using a sperm bank.
Modern surgical techniques increasingly utilize robotic assistance, enabling enhanced precision, smaller incisions, reduced blood loss, and faster recovery compared to traditional open surgery. The primary advantage of surgery lies in complete tumor removal, providing definitive pathological staging and potentially eliminating cancer with a single intervention.
About a quarter of those who had surgery reported urinary leakage after 10 years, compared with 11% who had radiation therapy. However, surgical techniques continue improving, with nerve-sparing approaches preserving erectile function when anatomically feasible.
Radiation Therapy: External and Internal Approaches
Radiation therapy uses high-energy beams to destroy cancer cells while sparing surrounding tissue. Multiple radiation modalities exist, each with distinct advantages.
External Beam Radiation Therapy (EBRT): Traditional EBRT delivers radiation from outside the body across multiple sessions. Until fairly recently, radiation therapy for prostate cancer was given 5 days a week for 8 weeks or even longer for a total of about 40 treatment sessions. However, treatment schedules have shortened dramatically.
Stereotactic Body Radiation Therapy (SBRT): SBRT treatment compresses therapy into just 5 sessions compared with the minimum of 20 that is often used, with men receiving SBRT not having a higher risk of cancer recurrence over the next 5 years than men treated with other commonly used radiation therapy regimens given over 4 to 8 weeks. This convenience dramatically reduces treatment burden.
Brachytherapy: This internal radiation approach places radioactive seeds directly into the prostate, delivering concentrated doses while minimizing exposure to surrounding tissues. High dose rate brachytherapy involves depositing high-dose radiation directly into the prostate through a catheter for 15-20 minutes, with outcomes showing disease-free survival rates in the 90%-95% range five years from treatment for patients with early-stage cancer.
Seven percent of men who had radiation plus hormone therapy reported serious bowel problems, compared with 2% to 5% of men who had surgery. This represents the primary trade-off between treatments—surgery more frequently affects urinary continence and erectile function, while radiation more commonly impacts bowel function.
Advanced Radiation Technologies
Recent technological advances have revolutionized radiation therapy precision and effectiveness. Proton therapy involves high-energy, precisely targeted particle beams that deposit radiation directly in the targeted tumor without exit dose beyond the targeted area, limiting collateral exposure to surrounding tissues and organs such as the bowel, rectum and bladder.
The SpaceOAR System represents another innovation addressing radiation therapy’s primary limitation. While radiation treatment has become more targeted, one of the biggest risks of radiation therapy of the prostate is injury to the rectum due to its proximity, with the SpaceOAR System providing a solution. This temporary gel creates space between prostate and rectum, reducing rectal radiation exposure.
Treatment Considerations for High-Risk and Locally Advanced Disease
Men with high-risk features or locally advanced cancer typically require more aggressive, multimodal approaches. Surgery has really improved a lot in the past 10 years with excellent quality of life, and a radical prostatectomy with a lymphadenectomy, mostly extended in the high-risk patient, has a big role especially in view of PSMA imaging data.
However, surgery alone may prove insufficient for high-risk disease. Many patients receive additional radiation therapy after surgery if pathological findings reveal concerning features. Salvage radiotherapy has been considered the only potentially curative therapy after biochemical failure and has been associated with better outcomes if given at lower PSA levels, with recent evidence showing salvage radiotherapy given at a PSA equal to or lower than 0.25 ng/mL is associated with improved all cancer-mortality.
Alternatively, radiation combined with hormone therapy represents a primary treatment option. The combination improves outcomes compared to radiation alone for high-risk patients, though it adds hormonal therapy side effects including hot flashes, decreased libido, fatigue, and potential bone density loss.
Metastatic Prostate Cancer: Systemic Approaches
When cancer spreads beyond regional lymph nodes to bones or distant organs, treatment focus shifts from cure to control and quality of life optimization. Hormone therapy (androgen deprivation therapy) forms the backbone of metastatic disease management, as most prostate cancers initially respond to testosterone suppression.
Modern systemic therapies include newer hormone agents, chemotherapy, immunotherapy, and radiopharmaceuticals. Radium-223, also known as liquid radiation, is administered through an IV infusion to patients with metastatic prostate cancer that has spread to the bones and has shown resistance to hormonal therapy. This targeted approach delivers radiation specifically to bone metastases while sparing other tissues.
PLUVICTO is indicated for treatment of men with prostate-specific membrane antigen-positive metastatic castration-resistant prostate cancer (PSMA-positive mCRPC), an option for someone whose cancer has spread to other parts of the body and who has already been treated with other anticancer treatments, administered intravenously every six weeks for up to six doses.
Frequently Asked Questions

What does my Gleason score mean, and how does it affect my treatment?
The Gleason score examines how cancer cells appear under microscopy compared to normal prostate cells. Scores range from 6 (least aggressive) to 10 (most aggressive), combining patterns of the two most common cell types in your biopsy. Grade Groups simplify this: Grade Group 1 (Gleason 6) represents the lowest risk, while Grade Group 5 (Gleason 9-10) indicates the highest. Your Gleason score profoundly influences treatment recommendations—Grade Group 1 might warrant active surveillance, whereas Grade Group 5 typically requires aggressive, multimodal therapy. Combined with PSA levels and T stage, your Grade Group determines your overall risk category and optimal treatment strategy.
Should I choose surgery or radiation therapy for my localized prostate cancer?
For prostate cancer that has not spread, surgery and radiation therapy have similar success rates, with doctors considering the cancer type and stage as well as a person’s overall health and preferences when choosing between the two. Neither treatment is universally “better”—the optimal choice depends on multiple factors including your age, overall health, other medical conditions, cancer characteristics, lifestyle priorities, and personal values regarding treatment duration, recovery time, and potential side effects. Many men with localized prostate cancer survive for 15 years or more with minimal differences in survival among various treatment strategies, so given this long-time horizon and similar survival rates, the choice of treatment may be influenced by the adverse effects of the treatments. Consult with both urologists and radiation oncologists to understand how each approach aligns with your priorities.
What is the difference between clinical and pathological staging?
Clinical staging (designated as cT) represents your doctor’s assessment before treatment, based on digital rectal exam, PSA levels, biopsy results, and imaging studies. Pathological staging (pT) occurs after surgery when the entire prostate is examined in the laboratory, providing definitive information about tumor size, extent, margins, and lymph node involvement. Pathological staging is more accurate because it’s based on direct tissue examination rather than estimates from tests. Sometimes pathological staging reveals cancer was more or less extensive than clinical staging suggested, potentially affecting decisions about additional therapy after surgery. This underscores why some men who appear to have favorable disease before surgery might still need postoperative radiation if pathological findings reveal concerning features.
Can I avoid treatment if my prostate cancer is low-risk?
Active surveillance represents a valid management strategy for carefully selected low-risk patients. This approach involves regular PSA testing (typically every 3-6 months), periodic digital rectal exams, and surveillance biopsies (often annually or every 1-2 years). Treatment begins only if monitoring detects disease progression—rising PSA levels, increasing tumor volume, or upgrading on biopsy. Active surveillance avoids treatment side effects while cancer remains indolent. Research demonstrates that appropriately selected patients on active surveillance have excellent survival outcomes comparable to immediate treatment. However, active surveillance requires psychological comfort living with untreated cancer and meticulous adherence to monitoring protocols. Discuss with your physician whether your specific cancer characteristics, age, overall health, and personal preferences make active surveillance appropriate.
How do I know if my cancer has spread?
Determining whether cancer has spread involves several tests. Bone scans or advanced imaging like PSMA PET scans detect bone metastases. CT scans or MRI evaluate lymph node involvement and soft tissue spread. Your PSA level provides clues—very elevated PSA (typically >20 ng/mL) increases metastasis likelihood, though lower levels don’t exclude spread. The decision about which imaging to perform depends on your cancer’s risk features: Grade Group, T stage, and PSA level. Low-risk patients rarely need extensive imaging, while high-risk features prompt comprehensive staging workup. Advanced imaging technologies like PSMA PET/CT demonstrate superior sensitivity for detecting metastatic disease compared to conventional bone and CT scans, potentially changing treatment approaches by identifying spread earlier.
What happens if my cancer comes back after treatment?
Biochemical recurrence—rising PSA after treatment—indicates cancer persistence or return before symptoms develop. Management depends on several factors: treatment received initially, timing of recurrence, PSA velocity, and whether recurrence is localized or distant. After surgery, rising PSA may prompt salvage radiation therapy to the prostate bed, most effective when PSA remains low. After radiation, salvage options include surgery, cryotherapy, or additional radiation, though these prove more challenging and carry higher complication risks. For some men, rising PSA despite local treatments indicates microscopic metastatic disease requiring systemic approaches like hormone therapy. Advanced imaging increasingly guides these decisions by localizing recurrence sites. Your oncology team will determine optimal management based on your specific circumstances, balancing treatment effectiveness against quality of life considerations.
How important is seeking a second opinion?
Seeking second opinions for prostate cancer diagnosis and treatment planning is not only reasonable but often recommended, particularly for intermediate- and high-risk disease. Prostate cancer management involves nuanced decisions weighing similar survival outcomes against different side effect profiles and quality of life impacts. Different specialists may emphasize different approaches—urologists may favor surgery while radiation oncologists champion radiation therapy. Seeking opinions from both specialties, preferably at centers with high prostate cancer treatment volumes, provides comprehensive perspective. Many cancer centers offer multidisciplinary clinics where patients meet multiple specialists in one visit, facilitating integrated treatment planning. Second opinions occasionally identify alternative diagnoses, reveal treatment options not initially discussed, or provide reassurance about recommended approaches. Most physicians welcome second opinions as part of informed decision-making rather than perceiving them as distrust.
Making Informed Treatment Decisions
The abundance of treatment options can feel overwhelming, but this variety enables personalized approaches matching your specific situation and priorities. Consider these factors when evaluating options:
Cancer Characteristics: Stage, Grade Group, PSA level, and risk category fundamentally guide appropriate treatment intensity.
Age and Life Expectancy: Younger men with decades of life expectancy may prioritize cure even if it risks side effects, while older men with limited life expectancy from other conditions might emphasize quality of life.
Overall Health: Other medical conditions influence surgical candidacy, anesthesia risks, and ability to tolerate multimodal therapies.
Personal Values: Your priorities regarding treatment side effects—urinary, bowel, and sexual function—deserve equal consideration alongside cancer control. Some men prioritize maintaining erectile function; others emphasize avoiding bowel problems; still others want the shortest treatment duration possible.
Support System: Recovery from surgery requires temporary assistance with daily activities, while radiation therapy demands reliable transportation for multiple appointments.
Professional and Lifestyle Considerations: Treatment timing may affect work responsibilities, caregiving obligations, or planned activities.
The Importance of Multidisciplinary Care
In bimonthly multidisciplinary clinics, a patient meets with a urology or radiation oncology resident or nurse practitioner, then the case is reviewed by a team including a urologic oncologist, a medical oncologist, a radiation oncologist, a radiologist and a pathologist, with each physician and the patient meeting in one-on-one sessions to discuss the best diagnosis and management options that afternoon. This collaborative approach ensures treatment recommendations reflect comprehensive expertise rather than single-specialty bias.
Seek care from institutions offering multidisciplinary evaluation, particularly for intermediate- or high-risk disease. The complexity of modern prostate cancer management—with advanced imaging, novel radiation techniques, emerging systemic therapies, and precision medicine approaches—requires expertise across multiple domains.
Conclusion
Understanding prostate cancer staging transforms an overwhelming diagnosis into a navigable journey. The TNM system, Grade Groups, PSA levels, and risk stratification provide the framework for personalized treatment decisions. Whether your situation calls for active surveillance, surgery, radiation, or systemic therapies, the goal remains the same: maximizing both quantity and quality of life.
The encouraging reality is that most men diagnosed with prostate cancer today will not die from their disease. Data from between 2013 and 2019 suggests that compared with people without prostate cancer, those with localized prostate cancer are more than 99% as likely to live for at least 5 years after their diagnosis. This outstanding prognosis reflects both screening effectiveness and treatment advances but also demands thoughtful decision-making to balance cancer control against treatment impacts on daily life.
Your prostate cancer journey is uniquely yours. Armed with staging knowledge, treatment understanding, and partnership with experienced oncology teams, you can confidently navigate decisions that honor both your medical needs and personal values. The wealth of effective treatment options means finding approaches aligned with your priorities while achieving excellent outcomes—the hallmark of modern, patient-centered prostate cancer care.


