
Discover critical leishmaniasis warning signs, powerful treatment options, and essential prevention strategies. Comprehensive guide to understanding this parasitic disease and protecting your health.
Introduction
Leishmaniasis affects approximately 12 million people worldwide, causing skin lesions, organ damage, and in severe cases, death if left untreated. This parasitic disease transmitted by sandfly bites remains one of the world’s most neglected tropical diseases, yet it’s spreading to new regions due to climate change, travel, and migration. If you’re planning to travel to endemic areas or live in affected regions, understanding leishmaniasis can literally save your life.
This comprehensive guide reveals everything you need to know about leishmaniasis, from recognizing warning signs to accessing effective treatments and implementing powerful prevention strategies.
Understanding Leishmaniasis: A Hidden Global Threat
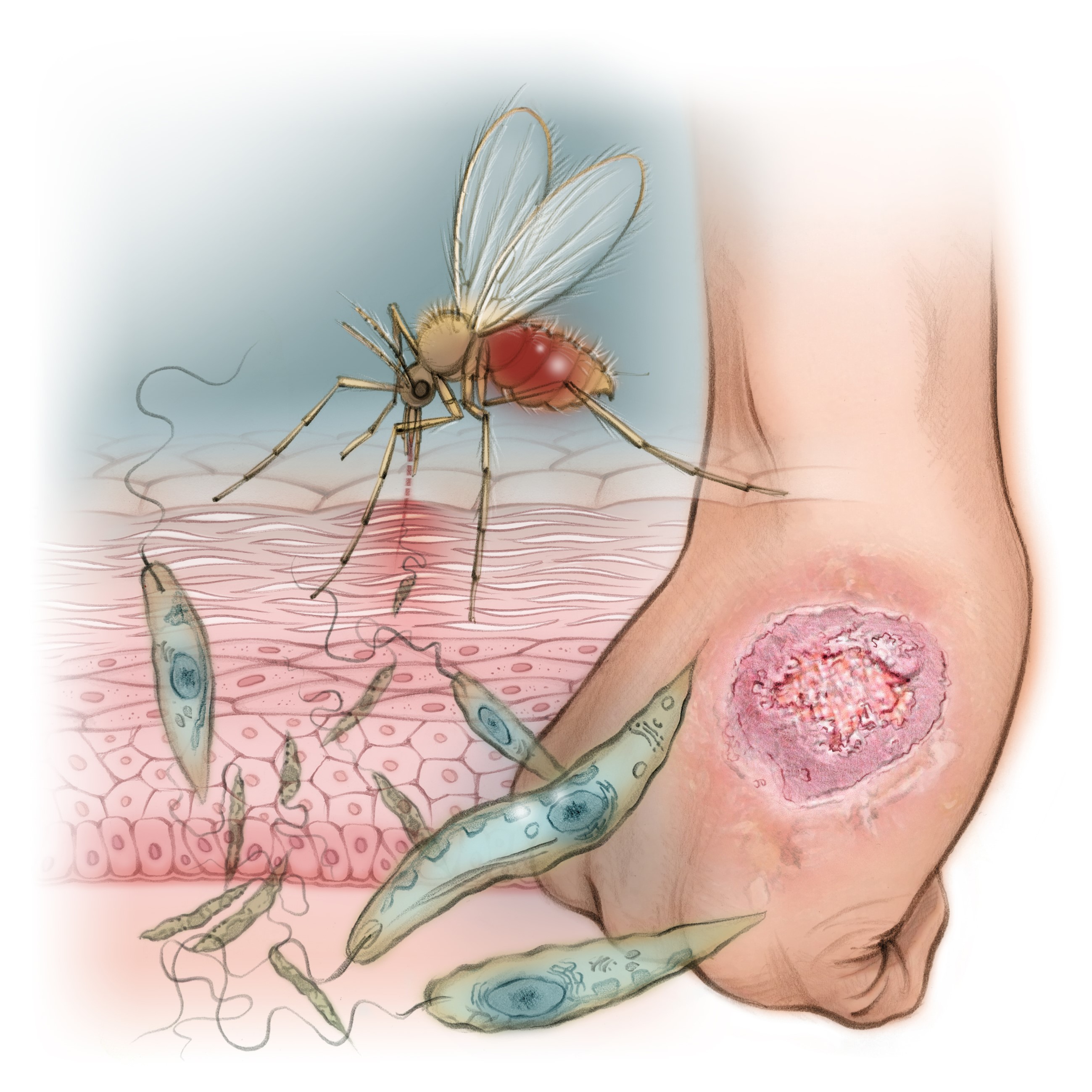
Leishmaniasis is a disease caused by Leishmania parasites transmitted to humans through the bites of infected female phlebotomine sandflies. These tiny insects—smaller than mosquitoes—breed in warm, humid environments and are most active from dusk to dawn.
The disease occurs primarily in tropical and subtropical regions of Africa, Asia, the Middle East, Central and South America, and southern Europe. Over 90 countries report leishmaniasis cases, with the poorest populations suffering disproportionately. Climate change is expanding sandfly habitats, bringing the disease to previously unaffected areas.
The Leishmania Life Cycle
When an infected sandfly bites, it injects Leishmania parasites into your skin along with saliva. The parasites invade immune cells called macrophages—cells normally responsible for destroying foreign invaders. Inside these cells, the parasites multiply and spread through the bloodstream or remain localized in skin tissue, depending on the species.
When another sandfly feeds on an infected person or animal, it ingests parasites, completing the transmission cycle. Domestic dogs, rodents, and wild animals serve as reservoir hosts, maintaining parasites in nature.
Types of Leishmaniasis
Cutaneous leishmaniasis (CL) is the most common form, causing skin sores at bite sites. These lesions may be painless or painful, single or multiple, and can leave permanent scars. CL accounts for approximately 95% of cases worldwide, with most occurring in Afghanistan, Algeria, Brazil, Colombia, Iran, and Syria.
Mucocutaneous leishmaniasis (MCL), a severe form, spreads from skin to mucous membranes of the nose, mouth, and throat. It causes extensive tissue destruction, facial disfigurement, and breathing difficulties. MCL occurs primarily in Bolivia, Brazil, and Peru.
Visceral leishmaniasis (VL), also called kala-azar, represents the most severe form. Parasites invade internal organs including the spleen, liver, and bone marrow. Without treatment, VL is fatal in over 95% of cases. Most VL cases occur in Brazil, East Africa, and the Indian subcontinent.
Post-kala-azar dermal leishmaniasis (PKDL) develops in some patients months to years after successful VL treatment, causing skin lesions despite parasite clearance from internal organs.
Recognizing Critical Warning Signs
Leishmaniasis symptoms vary dramatically based on disease type and individual immune response.
Cutaneous Leishmaniasis Symptoms
Skin lesions typically appear weeks to months after the sandfly bite, beginning as small papules (raised bumps) that gradually enlarge. These develop into nodules, then open ulcers with raised borders and central craters. Lesions may be painless or cause discomfort, and multiple lesions can occur from a single bite as parasites spread locally.
The appearance varies from small sores to large, disfiguring ulcers. Lymph nodes near lesions may swell. Without treatment, lesions may heal spontaneously over months to years, but often leave permanent scars. Some infections cause diffuse cutaneous leishmaniasis with widespread skin lesions resembling leprosy.
Mucocutaneous Leishmaniasis Symptoms
MCL typically begins with cutaneous lesions that may heal before mucosal involvement appears, sometimes years later. Early signs include persistent nasal congestion, nosebleeds, and nasal discharge. As the disease progresses, it causes destruction of nasal septum, perforation of the palate, lip swelling and ulceration, and severe facial disfigurement.
Without treatment, MCL causes breathing difficulties, eating problems, and secondary bacterial infections. The condition is life-altering, carrying significant social stigma and psychological impact on mental wellness.
Visceral Leishmaniasis Symptoms
VL has an incubation period ranging from weeks to months, occasionally years. Initial symptoms are often nonspecific, including irregular fever lasting weeks with high temperatures that come and go, progressive weakness and fatigue, significant weight loss and decreased appetite, and enlarged spleen and liver causing abdominal swelling.
Advanced VL causes severe anemia, low white blood cell counts increasing infection risk, bleeding problems from low platelets, darkening of skin (giving rise to the name kala-azar, meaning “black fever” in Hindi), and immune suppression making patients vulnerable to other infections.
VL in people with HIV/AIDS presents particular challenges, with higher treatment failure rates and increased mortality. Co-infection accelerates both HIV and leishmaniasis progression.
According to the World Health Organization, early diagnosis and treatment significantly improve outcomes, particularly for visceral leishmaniasis where delayed treatment proves fatal.
Comprehensive Diagnostic Approaches
Accurate diagnosis requires combining clinical assessment with laboratory confirmation, as symptoms often mimic other conditions.
Clinical Evaluation
Healthcare providers assess exposure history including travel to endemic areas, outdoor activities during sandfly active hours, animal contact, and living conditions. Physical examination documents lesion characteristics, size, number, and location for cutaneous disease, or organ enlargement and systemic symptoms for visceral disease.
Laboratory Diagnosis
For cutaneous leishmaniasis, tissue samples from lesion edges undergo microscopic examination to identify parasites. Culture of tissue samples in specialized media grows parasites for definitive identification. Molecular tests using PCR (polymerase chain reaction) detect parasite DNA with high sensitivity.
For visceral leishmaniasis, blood tests may show anemia, low white blood cells, and low platelets. Antibody tests detect immune response to parasites. Bone marrow, spleen, or lymph node aspirates provide samples for microscopic examination and culture, offering the most definitive diagnosis.
Rapid diagnostic tests using blood samples provide results in minutes, particularly valuable in resource-limited settings. Imaging with ultrasound or CT scans assesses spleen and liver enlargement.
Powerful Treatment Options That Save Lives
Treatment depends on leishmaniasis type, severity, location, and patient factors including immune status and pregnancy.
Cutaneous Leishmaniasis Treatment
Mild, single lesions in non-cosmetically sensitive areas may heal without treatment, though this risks spreading and scarring. Local therapies include intralesional antimonials injected directly into lesions, thermotherapy applying controlled heat to destroy parasites, and cryotherapy freezing lesions with liquid nitrogen.
Topical paromomycin ointment treats some cutaneous forms, particularly in the Old World (Africa, Asia, Middle East). Systemic treatments for multiple, large, or mucosal-risk lesions include pentavalent antimonials (sodium stibogluconate or meglumine antimoniate) given by injection for 10-20 days. These remain first-line treatment in many areas despite toxicity concerns.
Alternative systemic treatments include miltefosine, the first oral leishmaniasis drug, offering convenient outpatient treatment. Amphotericin B, particularly liposomal formulation, shows excellent efficacy with fewer side effects than antimonials. Pentamidine works for some species but carries significant toxicity.
Mucocutaneous Leishmaniasis Treatment
MCL requires aggressive systemic treatment, as local therapies prove inadequate. Extended courses of antimonials, liposomal amphotericin B, or combination therapies may be necessary. Surgical reconstruction may address severe tissue destruction after parasite elimination.
Visceral Leishmaniasis Treatment
VL requires immediate systemic treatment due to high mortality risk. Liposomal amphotericin B represents the preferred treatment in many regions, offering excellent efficacy with relatively low toxicity. The medication is given intravenously over several days.
Pentavalent antimonials, though older, remain widely used where liposomal amphotericin B isn’t available. These require 28-30 days of daily injections with careful monitoring for cardiac and pancreatic toxicity.
Miltefosine provides oral VL treatment, improving patient compliance and enabling home-based care. Paromomycin, an aminoglycoside antibiotic, works against VL, particularly when combined with antimonials.
Combination therapies—using two or three drugs simultaneously—shorten treatment duration, reduce toxicity, and may prevent drug resistance. Various combinations are being evaluated and implemented based on regional resistance patterns.
Supportive Care
All leishmaniasis patients benefit from nutritious diet supporting immune function and recovery. VL patients often require blood transfusions for severe anemia, antibiotics for secondary infections, and nutritional supplementation for severe malnutrition. Close monitoring during treatment identifies and manages drug side effects promptly.
Post-Treatment Follow-Up
Regular follow-up ensures complete cure and early detection of relapse or PKDL. For cutaneous disease, monitor lesion healing and scar formation. For visceral disease, repeat testing confirms parasite clearance and monitors for PKDL development.
Essential Prevention Strategies That Work
Preventing leishmaniasis focuses on avoiding sandfly bites and reducing sandfly populations in endemic areas.
Personal Protection Measures
Avoid outdoor activities from dusk to dawn when sandflies are most active, particularly in endemic areas. If you must be outdoors during these hours, take protective measures including wearing long sleeves, long pants, and socks to minimize exposed skin. Treat clothing with permethrin insecticide for added protection.
Apply insect repellent containing DEET, picaridin, or IR3535 to exposed skin. Reapply according to product instructions, especially after sweating or swimming. Use fine-mesh bed nets, ideally treated with insecticide. Sandflies are much smaller than mosquitoes, so standard mosquito nets may not provide adequate protection unless mesh is very fine.
Environmental Control
Reduce sandfly breeding sites by clearing organic debris, maintaining clean surroundings, and controlling rodent populations that serve as reservoir hosts. In endemic areas, residual insecticide spraying in houses and animal shelters reduces sandfly populations.
Travel Precautions
Research your destination before traveling to endemic areas. Understand local leishmaniasis risk and take appropriate precautions. Choose accommodations with air conditioning and window screens when possible, as sandflies are weak fliers and rarely enter well-screened or air-conditioned spaces.
Schedule outdoor activities during daytime hours. If camping, use properly treated bed nets and sleep elevated off the ground. Consider chemoprophylaxis (preventive medication) for high-risk travelers to highly endemic areas, though no universally approved prophylactic regimen exists.
Vaccination Development
No vaccine currently exists for human leishmaniasis, though research continues. Several candidates are in various development stages, offering hope for future prevention tools. Until then, bite prevention remains crucial.
Special Populations and Considerations
Immunocompromised Individuals
People with HIV/AIDS, organ transplant recipients, and those on immunosuppressive therapy face higher leishmaniasis risk and more severe disease. VL-HIV co-infection requires specialized treatment approaches and longer therapy duration. These individuals should take extra precautions in endemic areas and seek immediate evaluation for any suspicious symptoms.
Children
Children in endemic areas bear significant leishmaniasis burden. Pediatric treatment requires careful dose adjustment and monitoring. Cutaneous lesions in children may cause significant psychological distress and social problems, emphasizing the importance of preventive care.
Pregnant Women
Some leishmaniasis treatments are contraindicated during pregnancy due to teratogenic risks. Miltefosine, in particular, should not be used. Treatment decisions balance disease severity against potential fetal risks. Prevention is especially important for pregnant women in endemic areas.
Domestic Animals
Dogs serve as important reservoir hosts, particularly for visceral leishmaniasis. In endemic areas, protective measures for dogs include insecticide-treated collars, topical preventives, and in some regions, canine vaccines. Infected dogs may require treatment or, in some control programs, euthanasia to prevent transmission.
Living in Endemic Areas
Community Education
Understanding leishmaniasis transmission and prevention empowers communities to protect themselves. Public health education programs should emphasize recognizing symptoms, seeking early treatment, and implementing prevention measures.
Reducing Stigma
Leishmaniasis, particularly mucocutaneous and post-kala-azar forms, can cause disfiguring lesions leading to social stigma and isolation. Education reduces stigma and encourages treatment-seeking. Supporting affected individuals’ mental wellness is crucial for recovery and reintegration.
Economic Impact
Leishmaniasis disproportionately affects poor communities, creating vicious cycles of poverty and disease. The condition causes lost work productivity, expensive treatments, and long-term disability. Addressing leishmaniasis requires integrated approaches combining medical treatment, vector control, and socioeconomic development.
The Global Fight Against Leishmaniasis
Leishmaniasis remains classified as a neglected tropical disease despite affecting millions. Limited research funding, inadequate diagnostic tools in resource-poor settings, drug resistance emergence, and climate change expanding sandfly ranges all complicate control efforts.
International initiatives work toward leishmaniasis elimination in specific regions, improved diagnostic tools, more accessible and affordable treatments, and development of effective vaccines. Progress requires sustained commitment from governments, healthcare systems, and international organizations.
Frequently Asked Questions About Leishmaniasis
Can leishmaniasis spread from person to person?
No, leishmaniasis doesn’t spread through direct person-to-person contact, sexual contact, or casual contact like shaking hands. The disease requires sandfly vectors for transmission. However, it can spread through blood transfusions, shared needles, or congenitally from mother to fetus in rare cases. Infected individuals aren’t contagious in normal social interactions.
Is leishmaniasis curable?
Yes, leishmaniasis is curable with appropriate treatment. Cutaneous forms typically heal completely with treatment, though scars may remain. Visceral leishmaniasis responds well to modern treatments when diagnosed and treated promptly. However, delayed treatment, drug resistance, and immunocompromise can complicate cure. Post-kala-azar dermal leishmaniasis may require extended treatment courses.
How long after a sandfly bite do symptoms appear?
The incubation period varies widely. Cutaneous leishmaniasis typically appears weeks to months after the bite, though it can take up to a year. Visceral leishmaniasis has longer incubation, usually 2-6 months but potentially years. This delayed onset often obscures the connection between travel to endemic areas and disease onset.
Can you get leishmaniasis more than once?
Yes, reinfection can occur, though previous infection provides some immunity against the same species. Different Leishmania species can cause new infections. In endemic areas, residents may experience multiple episodes throughout their lives. Immunocompromised individuals face higher reinfection and relapse risks.
Do all sandfly bites cause leishmaniasis?
No, only sandflies infected with Leishmania parasites transmit disease. Even in endemic areas, the proportion of infected sandflies varies. Additionally, not everyone bitten by an infected sandfly develops disease—immune response and parasite load influence infection establishment. However, avoiding all sandfly bites remains the best prevention strategy.
Are leishmaniasis treatments expensive?
Treatment costs vary dramatically by location, disease type, and chosen therapy. In resource-limited endemic areas, many treatments are provided through public health programs or international organizations at reduced or no cost. In developed countries, treatments—particularly liposomal amphotericin B—can be expensive. Access to affordable treatment remains a significant global health challenge.
Can leishmaniasis be prevented with medication?
Currently, no approved preventive medication exists for leishmaniasis. Research has explored various chemoprophylaxis options, but none are widely recommended or used. Prevention focuses on avoiding sandfly bites through protective measures. A safe, effective vaccine would revolutionize prevention but remains under development.
How serious is leishmaniasis?
Seriousness varies by type. Cutaneous leishmaniasis, while causing disfiguring lesions and scars, is rarely fatal. Mucocutaneous leishmaniasis causes severe morbidity through tissue destruction and disfigurement. Visceral leishmaniasis is life-threatening, with over 95% mortality if untreated. However, early diagnosis and appropriate treatment dramatically improve outcomes even for visceral disease. The key is recognizing symptoms and seeking medical care promptly.

