Few diseases carry the psychological weight of Ebola. The name alone conjures images of remote jungle outbreaks, stricken communities, and overwhelmed health workers in full protective gear. For most people outside sub-Saharan Africa, Ebola feels distant, something that happens somewhere else. And yet in May 2026, the World Health Organization declared a Public Health Emergency of International Concern (PHEIC) over a fast-growing Ebola outbreak in the Democratic Republic of the Congo and Uganda, the second largest Ebola outbreak on record, with more than 1,000 confirmed cases as of late June 2026.
Understanding Ebola is no longer an academic exercise. The virus has now caused outbreaks across nearly 50 years of documented history, consistently demonstrating both its devastating potential and the power of coordinated public health response to contain it. The good news, and it is significant, is that medicine has changed the rules of the game. We now have approved vaccines and treatments that simply did not exist a decade ago.
In this post, we break down everything you need to know: what Ebola is, how it spreads, how it’s recognized and diagnosed, what treatments are now available, and what the current 2026 outbreak means for global health. Whether you’re a curious reader or planning travel to affected regions, this guide provides the facts you need.
| 25–90%Case fatality rate range across outbreaks | ~50%Average CFR historically | 1,000+Confirmed cases, 2026 DRC/Uganda outbreak (as of June 22) | 1976Year Ebola was first identified |
What is Ebola disease?
Ebola virus disease (EVD), formerly known as Ebola hemorrhagic fever, is a rare but severe, often fatal illness in humans caused by viruses of the genus Ebolavirus. It belongs to the filovirus family, a group of RNA viruses that cause hemorrhagic fever syndromes in humans and other primates.
There are six recognized species of ebolavirus, four of which cause disease in humans:
- Zaire ebolavirus (EBOV), the most dangerous and most frequently causing outbreaks; responsible for the 2014–2016 West Africa epidemic and the DRC’s most recent Zaire outbreaks
- Sudan ebolavirus (SUDV), the cause of Uganda’s January 2025 outbreak (declared over April 2025)
- Bundibugyo ebolavirus (BDBV), the cause of the active 2026 DRC/Uganda outbreak; two prior outbreaks in 2007 and 2012
- Taï Forest ebolavirus (TAFV), very rare; one known human case
A critical point for 2026: approved vaccines and treatments only protect against Zaire ebolavirus. The current Bundibugyo-strain outbreak has no licensed vaccine and no approved therapeutic, only supportive care. This is one reason the WHO declared a PHEIC.
See our related post on how the immune system fights viral infection for background on the biological principles underlying Ebola’s severity.
How does Ebola spread?
One of the most important, and most misunderstood, facts about Ebola is how it doesn’t spread. Ebola is not airborne. There are no documented cases of Ebola transmission between humans or other primates through the air. This fundamentally limits its spread compared to respiratory viruses like influenza or COVID-19.
Animal-to-human (zoonotic) transmission
Ebola is a zoonotic disease, it originates in animals and crosses into humans. Fruit bats are believed to be the natural reservoir host, carrying the virus without becoming ill. Humans become infected through close contact with the blood, secretions, organs, or bodily fluids of infected animals, including bats, non-human primates (chimpanzees, gorillas), porcupines, and possibly domestic pigs. This initial spillover event is how outbreaks begin.
Areas undergoing deforestation face elevated risk because habitat destruction brings wildlife into closer contact with human settlements, a pattern that has repeatedly preceded outbreak events.
Human-to-human transmission

Once the virus enters a human host, it spreads through direct contact with the blood, bodily fluids, secretions, organs, or contaminated materials (bedding, clothing, needles) of a symptomatic person. Crucially, an infected person is not contagious until symptoms appear.
Persistence after recovery: Ebola virus can persist in semen for up to 12 months and in breast milk for several weeks after a person recovers. Sexual transmission from survivors has been documented and is an important driver of late-stage outbreak amplification.
Healthcare workers face disproportionate risk when proper infection prevention and control (IPC) measures are not in place. In the 2025 DRC Kasai outbreak, 5 of 53 confirmed cases were healthcare workers. Unsafe burial practices, where mourners come into contact with the body of someone who died of Ebola, have historically been a significant transmission route.
Signs and symptoms: what to watch for
The incubation period, the time between infection and the appearance of symptoms, ranges from 2 to 21 days, with most cases appearing within 8–10 days. A person is not contagious during this window, which is why contact tracing over a 21-day monitoring period is the cornerstone of outbreak control.
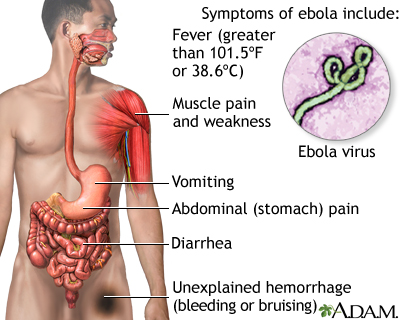
Early symptoms (days 1–5)
The onset of Ebola symptoms is sudden and initially resembles many other common illnesses:
- High fever
- Severe headache
- Muscle pain and weakness
- Sore throat
- Fatigue
This non-specific presentation makes early clinical diagnosis extremely difficult. Ebola symptoms at this stage are almost indistinguishable from malaria, typhoid fever, meningitis, or other viral hemorrhagic fevers, which is why laboratory testing is essential.
Later symptoms (days 5 onwards)
- Vomiting and diarrhea (often severe and watery)
- Rash
- Impaired kidney and liver function
- In some cases: internal and external bleeding, oozing from gums, blood in stool, nosebleeds, vomiting blood
Laboratory findings typically show low white blood cell and platelet counts alongside elevated liver enzymes. Death, when it occurs, usually results from shock caused by fluid loss, typically between 6 and 16 days after symptom onset.
Seek immediate care if you have traveled to an affected region and develop these symptoms within 21 days of return. Notify the healthcare facility before arrival so they can implement appropriate precautions.
Diagnosis: how Ebola is confirmed
Because early Ebola symptoms mimic so many other conditions, clinical diagnosis alone is insufficient. Confirmation requires laboratory testing. The standard approach is:
- RT-PCR (reverse transcription polymerase chain reaction), detects Ebola viral RNA in blood samples; the gold standard for confirmation
- Antigen-capture ELISA, detects Ebola proteins; useful in field settings
- IgM and IgG antibody detection, used in later-stage or post-recovery testing
- Rapid diagnostic tests (RDTs), increasingly used at outbreak epicenters for faster field-level results, validated against RT-PCR per 2024 WHO guidance
Blood samples from suspected Ebola patients are considered an extreme biohazard and must be handled under maximum (BSL-4) biosafety conditions. Sample collection, packaging, and transport are governed by strict WHO protocols updated in 2024.
Treatment: what medicine can now offer
The treatment landscape for Ebola has changed dramatically since the 2014–2016 West Africa epidemic. Here is where things stand in 2026.
Supportive care (all strains)
For all forms of Ebola, regardless of strain, aggressive supportive care significantly improves survival. This includes intravenous fluid and electrolyte repletion, oxygen support, pain management, treatment of secondary infections, and careful nutritional support. Early access to supportive care, ideally in a dedicated Ebola treatment center, can meaningfully shift outcomes. WHO issued updated clinical care guidelines in 2023.
Approved monoclonal antibodies (Zaire strain only)
Two targeted treatments are FDA-approved, both only for Zaire ebolavirus:
- Inmazeb (atoltivimab, maftivimab, odesivimab-ebgn), a triple monoclonal antibody cocktail approved in October 2020. Demonstrated improved 28-day survival versus the previous standard in the landmark PALM trial (2018–2020 DRC outbreak).
- Ebanga (ansuvimab), a single monoclonal antibody, also approved in December 2020. Showed comparable survival benefit in the same PALM randomized trial. WHO issued a strong recommendation for both in its first-ever EVD therapeutics guideline (August 2022).
Important limitation: The efficacy of Inmazeb and Ebanga has not been established for Sudan, Bundibugyo, or Taï Forest ebolavirus. Patients in the current 2026 Bundibugyo outbreak have no approved targeted therapy available, only supportive care while investigational options are considered under emergency frameworks.
Vaccines (Zaire strain only)
Ervebo (rVSV-ZEBOV) is the only FDA-approved vaccine for Ebola prevention, licensed in December 2019. It protects against Zaire ebolavirus and is deployed using a ring vaccination strategy, vaccinating contacts and contacts-of-contacts of confirmed cases to create a protective buffer around the outbreak. Over 47,000 doses were administered during the 2025 DRC Kasai outbreak. Protection is believed to last several years, though it may decrease over time.
Critical gap: There are currently no licensed vaccines for Sudan or Bundibugyo ebolavirus. Several candidate vaccines for these strains are in development, and the 2026 PHEIC is likely to accelerate their development timelines.
The 2026 outbreak: what you need to know
The current situation represents the most serious Ebola crisis in nearly a decade. Here is a chronology of recent EVD events:
| Date | Event | Strain | Status |
| Jan–Apr 2025 | Uganda (Sudan virus), Kampala; 14 cases, 4 deaths | Sudan | Declared over Apr 26, 2025 |
| Sep–Dec 2025 | DRC Kasai Province (Zaire); 64 cases, 45 deaths (CFR 70.3%) | Zaire | Declared over Dec 1, 2025 |
| May 2026 (ongoing) | DRC Ituri Province + Uganda (Bundibugyo); 1,000+ confirmed cases as of June 22; second largest EVD outbreak on record | Bundibugyo | Active, PHEIC declared May 17, 2026 |
The 2026 outbreak has spread from Ituri Province in northeastern DRC into Uganda, including cases in the capital Kampala. The Africa CDC has identified 10 surrounding countries at high risk. The CDC has issued travel health notices for DRC and Uganda and is routing affected air travelers through four designated U.S. airports for enhanced health screening. The current outbreak is growing faster than any previous Ebola outbreak on record.
Travel advisory: The CDC recommends avoiding non-essential travel to Ituri, Nord-Kivu, and Sud-Kivu provinces in DRC. Check current advisories at cdc.gov/ebola before any travel to the region.
Prevention and outbreak control
In the absence of a licensed vaccine for the Bundibugyo strain, outbreak control depends on a coordinated package of public health measures that have proven effective across decades of response:
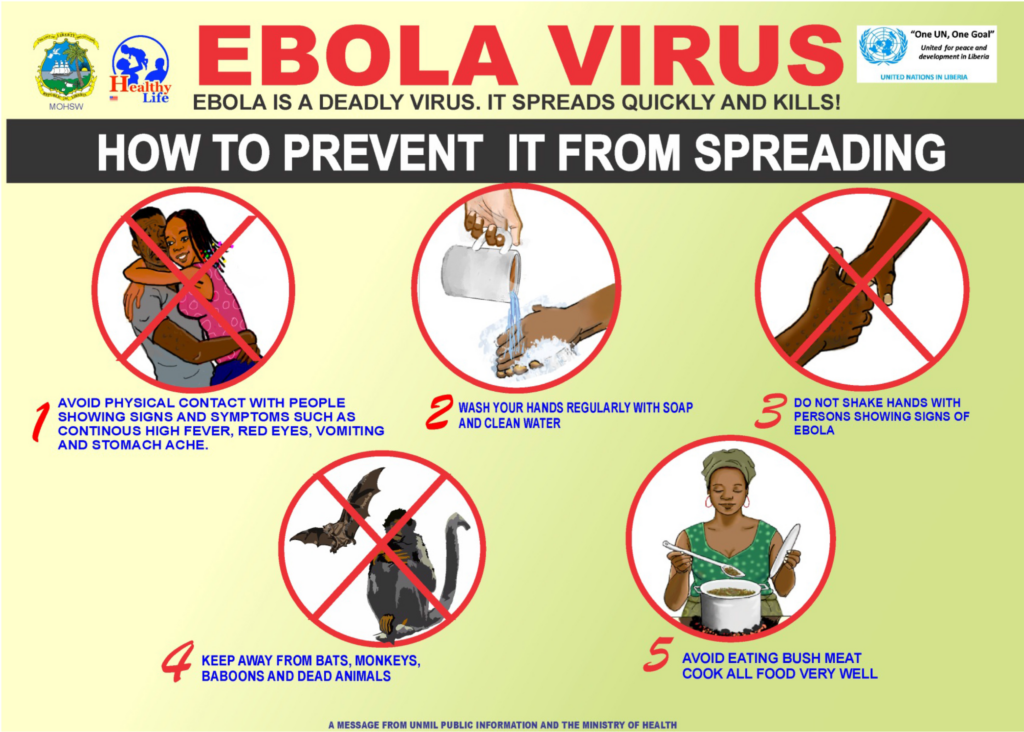
- Rapid case detection, identifying and isolating cases quickly to interrupt transmission chains
- Contact tracing, following up all known contacts of confirmed cases over 21 days
- Infection prevention and control (IPC) in healthcare facilities, proper personal protective equipment (PPE), triage protocols, and decontamination procedures
- Safe and dignified burials, burial teams trained to handle Ebola-positive bodies safely, respecting cultural practices where possible
- Community engagement, building trust with affected communities to overcome hesitancy and misinformation; historically one of the most critical success factors
- Laboratory capacity, maintaining rapid diagnostic capability near outbreak epicenters
For individuals outside outbreak zones, the global risk remains low. Ebola does not spread through casual contact, air travel, or food. The risk to the general American public from the current outbreak is considered low by the CDC, though surveillance at points of entry has been significantly strengthened.
Living as a survivor: long-term effects
Surviving Ebola is not the end of the medical journey. A significant proportion of survivors, in some studies, the majority, experience a constellation of long-term symptoms collectively called Post-Ebola Virus Disease Syndrome (PEVDS). These include:
- Joint and muscle pain
- Headaches
- Eye problems, including uveitis, which can lead to vision loss
- Hearing loss
- Fatigue and sleep disturbances
- Mental health challenges, including depression, PTSD, and anxiety
Survivors also carry Ebola virus in certain immune-privileged sites (semen, eyes) for months after clinical recovery, requiring careful follow-up and guidance on safe sexual practices. WHO published updated clinical care guidelines for EVD survivors in 2022. Survivor care programs are a recognized component of outbreak response. See our post on mental health support during serious illness for additional resources.
Key takeaways
- Ebola is not airborne. It spreads through direct contact with bodily fluids of a symptomatic person, not through casual contact or air travel. Understanding this prevents both complacency and unwarranted panic.
- A WHO PHEIC was declared in May 2026 for a Bundibugyo-strain outbreak in DRC and Uganda, the second largest Ebola outbreak in history, with 1,000+ cases and no licensed vaccine or treatment for this specific strain.
- Approved medical countermeasures exist for Zaire ebolavirus only, Ervebo vaccine, and monoclonal antibodies Inmazeb and Ebanga. These do not cover the active 2026 Bundibugyo outbreak.
- Early supportive care dramatically improves survival across all strains. Getting to a treatment center quickly, and early community reporting, saves lives.
- If you have traveled to an affected region and develop fever, headache, or muscle pain within 21 days, seek medical care immediately and inform the facility of your travel history before arrival.
Closing: fear is not the answer, preparedness is
Ebola is one of the most frightening words in global health, and one of the most misunderstood. It is deadly, yes. But it is also slow-spreading relative to respiratory viruses, well-characterized by decades of research, and increasingly responsive to medical intervention. The system that failed so catastrophically in West Africa in 2014, catching the outbreak late, responding slowly, lacking effective tools, is not the system we have in 2026. Response frameworks are stronger, diagnostics faster, and medical options far more advanced.
The 2026 Bundibugyo outbreak is a serious challenge, made harder by the absence of licensed countermeasures for this strain. But it is also a moment that will likely accelerate vaccine and therapeutic development for the strains that have so far been left behind. Stay informed through authoritative sources: WHO Ebola Fact Sheet and CDC Ebola Situation Summary are updated regularly. And explore more on ChiidHealth.com: how the immune system is being harnessed in medicine | gene therapy and the future of infectious disease | how vaccines work.

