Comprehensive guide to chronic lymphocytic leukemia (CLL). Discover symptoms, stages, cutting-edge treatment options, survival rates, and expert strategies for managing this blood cancer effectively.
Introduction
Receiving a chronic lymphocytic leukemia diagnosis can feel overwhelming, filling you with questions, fears, and uncertainty about the future. Yet understanding this condition—the most common type of leukemia in adults—empowers you to make informed decisions, access optimal treatments, and maintain quality of life. With advancing therapies and personalized treatment approaches, many people with chronic lymphocytic leukemia live full, active lives for years or even decades after diagnosis.
What Is Chronic Lymphocytic Leukemia?
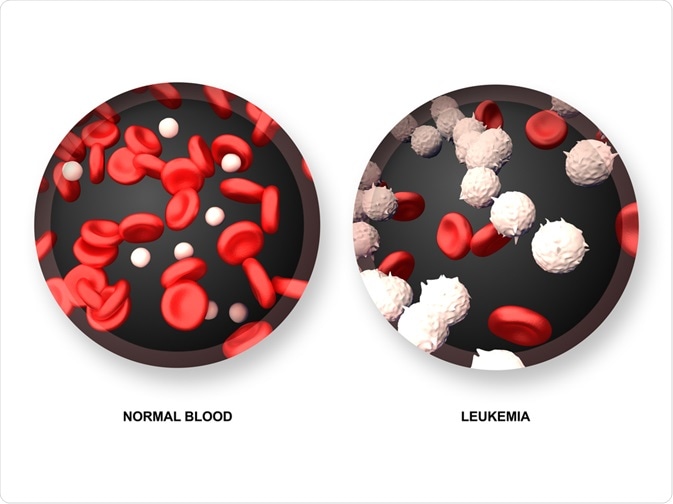
Chronic lymphocytic leukemia (CLL) is a slow-growing cancer affecting lymphocytes, a type of white blood cell crucial for fighting infections. In CLL, your bone marrow produces abnormally high numbers of defective lymphocytes that cannot function properly. These cancerous cells accumulate in your blood, bone marrow, lymph nodes, and spleen, gradually crowding out healthy blood cells.
Unlike acute leukemias that develop rapidly and require immediate treatment, CLL progresses slowly, often over years. This characteristic gives the disease its “chronic” designation. Many people with early-stage CLL experience no symptoms for extended periods and may not require immediate treatment—a management approach called “watchful waiting.”
Understanding Lymphocytes:
Lymphocytes form a vital part of your immune system, defending against infections and diseases. Two main types exist: B lymphocytes (B cells) produce antibodies that attack bacteria and viruses, while T lymphocytes (T cells) directly destroy infected or abnormal cells. CLL most commonly affects B cells, though rare T-cell variants exist.
In CLL, genetic mutations cause lymphocytes to multiply uncontrollably and survive much longer than normal cells. These defective cells cannot effectively fight infections, leaving you vulnerable to various illnesses despite having elevated white blood cell counts.
Recognizing Symptoms: Warning Signs of CLL
Early Stage Symptoms:
Many people with CLL experience no symptoms initially, with the condition discovered incidentally during routine blood work for unrelated reasons. This asymptomatic period may last months or years.
When symptoms do appear, they often develop gradually and may include:
Swollen Lymph Nodes: Painless enlargement of lymph nodes in your neck, armpits, or groin—often the first noticeable sign. These swellings feel firm and rubbery rather than tender.
Fatigue: Persistent tiredness unrelieved by rest, resulting from anemia as cancerous cells crowd out red blood cell production.
Frequent Infections: Recurring respiratory infections, urinary tract infections, or skin infections due to compromised immune function.
Unintentional Weight Loss: Losing 10% or more of body weight without trying within six months.
Fever and Night Sweats: Unexplained fevers or drenching night sweats requiring clothing changes.
Advanced Stage Symptoms:
As CLL progresses, additional symptoms may emerge:
- Easy bruising or bleeding from low platelet counts
- Shortness of breath during normal activities
- Feeling full quickly or abdominal discomfort from enlarged spleen
- Bone pain or tenderness
- Pale skin from severe anemia
Similar to how recognizing blood disorder symptoms requires awareness, identifying CLL warning signs enables timely medical evaluation.
Risk Factors: Who Develops CLL?
Age:
CLL predominantly affects older adults, with most diagnoses occurring after age 60. The condition rarely develops in people under 40.
Gender:
Men develop CLL approximately twice as frequently as women, though reasons for this disparity remain unclear.
Race and Ethnicity:
White individuals have higher CLL rates compared to Asian or African populations. People of Ashkenazi Jewish descent face particularly elevated risk.
Family History:
Having close relatives with CLL or other blood cancers increases your risk. Research suggests genetic factors contribute significantly to CLL development.
Chemical Exposure:
Prolonged exposure to certain herbicides, pesticides, and industrial chemicals may increase risk, though evidence remains somewhat limited. This environmental concern parallels risks associated with pesticide health exposure.
Agent Orange Exposure:
Veterans exposed to Agent Orange during Vietnam service face elevated CLL risk, now recognized as a service-connected condition.
Diagnosis: How Doctors Identify CLL
Complete Blood Count (CBC):
This initial screening test measures different blood cell types. CLL typically shows elevated lymphocyte counts, often dramatically higher than normal ranges. Abnormal CBC results trigger further investigation.
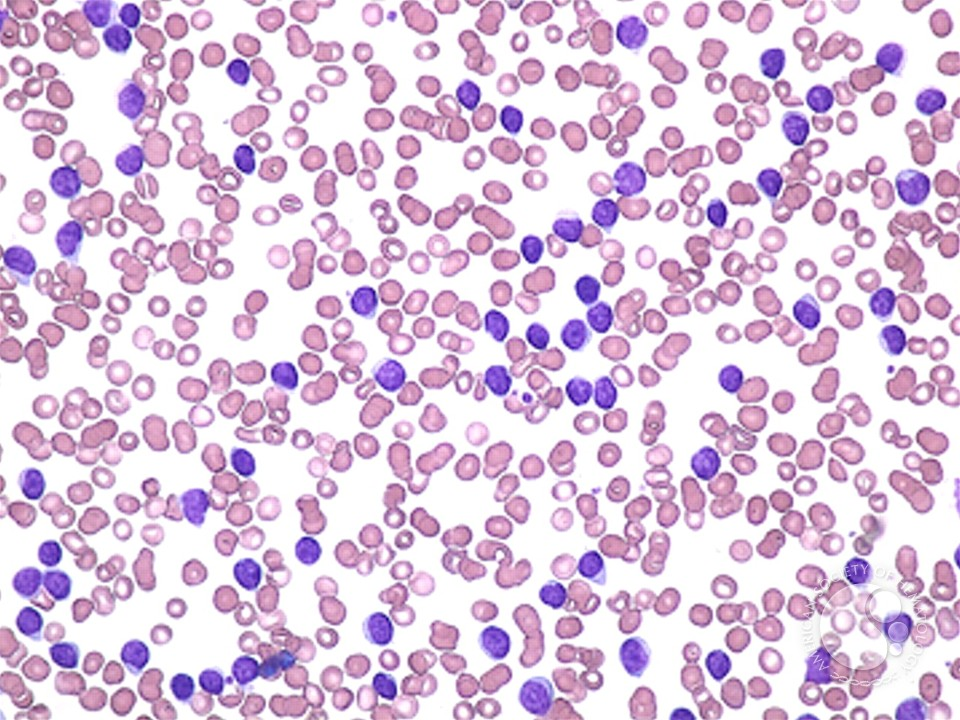
Blood Smear:
Laboratory technicians examine blood samples under microscope, identifying characteristic CLL cell appearance and distinguishing it from other conditions.
Immunophenotyping (Flow Cytometry):
This sophisticated test analyzes specific proteins on lymphocyte surfaces, confirming CLL diagnosis and differentiating it from similar blood cancers. The test identifies characteristic CLL markers including CD5, CD19, and CD23.
Genetic Testing:
Fluorescence In Situ Hybridization (FISH): Detects chromosomal abnormalities affecting prognosis and treatment selection. Common abnormalities include deletions of chromosomes 13q, 11q, and 17p.
Immunoglobulin Heavy Chain Variable Region (IGHV) Gene Mutation Status: Determines whether CLL cells have mutated or unmutated IGHV genes, significantly impacting disease progression rate and treatment response.
Bone Marrow Biopsy:
While not always necessary for CLL diagnosis, bone marrow examination may be performed to assess disease extent or investigate unclear cases.
Imaging Studies:
CT scans or ultrasound may evaluate lymph node, liver, and spleen enlargement, helping determine disease stage.
According to the Leukemia & Lymphoma Society, accurate diagnosis and staging guide treatment decisions and predict outcomes.
Staging: Understanding Disease Progression
Two main staging systems classify CLL severity:
Rai Staging System (United States):
- Stage 0: Lymphocytosis only (elevated lymphocyte counts)
- Stage I: Lymphocytosis plus enlarged lymph nodes
- Stage II: Lymphocytosis plus enlarged spleen or liver
- Stage III: Lymphocytosis plus anemia (low red blood cells)
- Stage IV: Lymphocytosis plus thrombocytopenia (low platelets)
Binet Staging System (Europe):
- Stage A: Fewer than three areas of lymphoid tissue enlargement
- Stage B: Three or more areas of lymphoid tissue enlargement
- Stage C: Anemia or thrombocytopenia present
Lower stages (Rai 0-I, Binet A) indicate slower progression and better prognosis, while higher stages require more aggressive monitoring or treatment.
Treatment Options: Fighting CLL Effectively
Watchful Waiting:
For early-stage, asymptomatic CLL, doctors often recommend observation without immediate treatment. This approach involves regular monitoring through physical exams and blood tests, initiating treatment only when symptoms develop or disease progresses. Research shows no survival benefit from treating asymptomatic early-stage CLL immediately.
Targeted Therapy:
Modern CLL treatment increasingly relies on targeted drugs attacking specific cancer cell characteristics:
BTK Inhibitors: Medications like ibrutinib, acalabrutinib, and zanubrutinib block Bruton’s tyrosine kinase, a protein essential for CLL cell survival and growth. These oral medications often produce dramatic, durable responses with manageable side effects.
BCL-2 Inhibitors: Venetoclax targets BCL-2 protein that helps cancer cells avoid death, often combined with antibody therapy for enhanced effectiveness.
PI3K Inhibitors: Drugs like idelalisib and duvelisib block PI3K enzyme, disrupting signals promoting cancer cell survival.
Immunotherapy:
Monoclonal Antibodies: Laboratory-created antibodies targeting specific proteins on CLL cells:
- Rituximab, obinutuzumab, and ofatumumab attach to CD20 protein on CLL cells, marking them for immune system destruction
- Often combined with chemotherapy or targeted therapy for improved results
CAR T-Cell Therapy: Revolutionary treatment extracting your T cells, genetically modifying them to recognize and attack CLL cells, then infusing them back into your body. Reserved for relapsed or treatment-resistant CLL.
Chemotherapy:
While less commonly used now than previously, chemotherapy remains valuable for certain patients:
- Fludarabine, cyclophosphamide, and bendamustine are commonly used agents
- Often combined with rituximab (FCR or BR regimens)
- Generally more effective in patients with mutated IGHV genes
Stem Cell Transplantation:
Allogeneic stem cell transplantation offers potential cure but carries significant risks. Reserved for younger patients with aggressive disease not responding to other treatments.
Supportive Care:
Managing complications remains crucial:
- Antibiotics preventing or treating infections
- Blood transfusions for severe anemia
- Growth factors stimulating blood cell production
- Immunoglobulin replacement therapy for recurrent infections
Similar to comprehensive approaches for chronic respiratory disease management, CLL treatment requires coordinated care addressing multiple aspects.
Prognosis and Survival Rates
CLL prognosis varies significantly based on multiple factors:
Five-Year Survival Rates:
Overall five-year relative survival rate for CLL exceeds 85%, though individual prognosis depends on specific characteristics:
- Early-stage disease (Rai 0): Over 95% five-year survival
- Intermediate stage (Rai I-II): 70-90% five-year survival
- Advanced stage (Rai III-IV): 60-70% five-year survival
Prognostic Factors:
Favorable: Mutated IGHV genes, isolated 13q deletion, normal karyotype
Unfavorable: Unmutated IGHV genes, 17p deletion, TP53 mutation, complex karyotype
Modern targeted therapies dramatically improve outcomes, particularly for previously hard-to-treat patient groups.
Living With CLL: Quality of Life Management
Infection Prevention:
With compromised immunity, preventing infections becomes paramount:
- Practice meticulous hand hygiene
- Avoid crowds during flu season
- Stay current with vaccinations (flu, pneumonia, COVID-19)
- Promptly report fever or infection signs to your doctor
- Consider prophylactic antibiotics if recommended
Nutrition and Exercise:
Maintain balanced nutrition for health optimization and engage in regular physical activity as tolerated. Exercise combats fatigue, maintains strength, and improves emotional wellbeing.
Emotional Support:
Cancer diagnosis triggers emotional challenges. Seek support through:
- Professional counseling or therapy
- Support groups connecting you with others facing CLL
- Open communication with family and friends
- Stress management techniques like meditation or yoga
The importance of mental health support cannot be overstated when facing chronic illness.
Regular Monitoring:
Attend all scheduled appointments, complete recommended blood work, and communicate changes in symptoms promptly.
Frequently Asked Questions About Chronic Lymphocytic Leukemia
Is chronic lymphocytic leukemia curable?
While CLL is generally considered incurable with standard treatments, many patients live for decades with excellent quality of life through ongoing management. Allogeneic stem cell transplantation offers potential cure but suits only select younger patients due to significant risks. Emerging therapies continue improving outcomes, and some patients achieve long-term remissions lasting years. The goal focuses on controlling disease, maintaining quality of life, and maximizing survival rather than necessarily achieving cure.
How quickly does CLL progress?
CLL progression varies tremendously between individuals. Some patients have very slow-growing disease remaining stable for years without requiring treatment, while others experience more rapid progression necessitating earlier intervention. Genetic markers like IGHV mutation status and chromosomal abnormalities help predict progression rates. Regular monitoring tracks disease activity, with treatment initiated when specific criteria indicating progression are met.
Can I work while being treated for CLL?
Many CLL patients continue working during treatment, particularly with modern targeted therapies causing fewer severe side effects than traditional chemotherapy. Work capacity depends on disease stage, treatment type, side effects experienced, and job physical demands. Some people work full-time throughout treatment, others reduce hours, and some take medical leave. Discuss your situation with your healthcare team and employer to develop appropriate accommodations.
Will I need treatment immediately after diagnosis?
Not necessarily. Many newly diagnosed CLL patients, particularly those with early-stage asymptomatic disease, enter watchful waiting rather than immediate treatment. Studies show no survival benefit from treating early-stage CLL before symptoms develop. Treatment begins when specific indications arise: progressive anemia or thrombocytopenia, enlarging lymph nodes causing problems, worsening symptoms, or evidence of rapidly progressive disease. Your hematologist determines optimal treatment timing.
What lifestyle changes should I make after CLL diagnosis?
Focus on infection prevention through hand hygiene, avoiding sick contacts, and maintaining vaccinations. Adopt healthy lifestyle habits including balanced nutrition, regular exercise as tolerated, adequate sleep, and stress management. Avoid tobacco and limit alcohol consumption. Stay well-hydrated and maintain good oral hygiene to prevent infections. Report any fever, unusual bleeding, or infection signs promptly. Continue routine health maintenance including dental care and cancer screenings. These changes support overall health and treatment effectiveness.
Hope Through Knowledge and Advanced Care
Chronic lymphocytic leukemia diagnosis undoubtedly represents a significant life challenge, but remarkable treatment advances offer genuine hope for long-term survival and quality of life. Understanding your disease, actively participating in treatment decisions, and maintaining open communication with your healthcare team position you for optimal outcomes.
CLL research continues advancing rapidly, with new therapies emerging regularly and survival rates steadily improving. Many patients live normal lifespans, particularly when disease remains indolent or responds well to treatment. By staying informed, adhering to treatment plans, practicing excellent self-care, and maintaining positive outlook, you maximize your chances for prolonged survival and meaningful life.
If you’ve been diagnosed with CLL or experience concerning symptoms, partner closely with experienced hematologists specializing in blood cancers. Their expertise, combined with your active engagement, creates the foundation for successfully navigating this journey. Remember, you’re not alone—comprehensive support systems exist to guide you every step of the way.

