What if, instead of poisoning cancer cells with chemicals or burning them with radiation, your doctor could simply train your own immune system to find and destroy them? That’s not science fiction, it’s immunotherapy, and it has fundamentally changed what’s possible in cancer treatment over the last decade.
The figures speak for themselves. Cancer remains one of the most significant health challenges of our time, with an estimated 2 million new cases and over 618,000 predicted deaths in the United States in 2025 alone. Yet cancer mortality has dropped by 31% since 1991, and immunotherapy is one of the key reasons why. Cancers that once had no effective treatment options, like advanced melanoma and certain lung cancers, now have patients achieving long-term remission, sometimes for years. A handful are even being declared cured.
But immunotherapy is also widely misunderstood. People hear about it from news headlines or other patients and assume it’s either a miracle cure available to everyone or a distant, experimental hope. The truth sits somewhere between those two extremes. In this post, we’ll walk you through what immunotherapy actually is, the different types now available, what the latest research shows about effectiveness, what side effects to expect, and how to know whether it might be an option for you or someone you love.
What Is Immunotherapy?
Immunotherapy is a type of cancer treatment that works by enhancing, directing, or restoring the body’s own immune system to recognize and attack cancer cells. Rather than targeting the tumor directly (as chemotherapy and radiation do), immunotherapy targets the relationship between your immune system and the cancer.
Your immune system is designed to detect and destroy abnormal cells, including cancerous ones. But cancer is cunning. Over time, tumors can develop strategies to hide from immune cells, suppress immune activity, and create an environment that shields them from attack. Immunotherapy aims to interrupt these evasion strategies and restore the immune system’s ability to do its job.
This is a fundamentally different philosophy from traditional cancer treatment, and it has opened the door to remarkable outcomes in cancers that previously had very limited options.
Immunotherapy is used to treat a growing range of cancers including melanoma, lung cancer, bladder cancer, head and neck cancers, kidney cancer, certain types of lymphoma, and some breast and colon cancers. It can be used alone or, increasingly, in combination with chemotherapy, radiation, or targeted therapies. See our post on tonsil cancer and immunotherapy for an example of how it’s being applied to head and neck cancers.
The Main Types of Immunotherapy
“Immunotherapy” is an umbrella term covering several distinct approaches, each working in a different way. Understanding the differences helps make sense of what you might read in clinical reports or hear from an oncologist.
Immune Checkpoint Inhibitors (ICIs)
Checkpoint inhibitors are currently the most widely used form of cancer immunotherapy. They work by blocking proteins, called checkpoints, that cancer cells use to disguise themselves as harmless, essentially tricking T-cells (your immune system’s attack cells) into standing down.
The most important checkpoints targeted by current drugs are:
- PD-1 / PD-L1, Cancer cells express a protein called PD-L1 that links to PD-1 on T-cells, effectively telling them “don’t attack me.” Drugs like pembrolizumab (Keytruda) and nivolumab (Opdivo) block this interaction, unmasking the cancer so T-cells can recognize and destroy it.
- CTLA-4, Another checkpoint protein that limits T-cell activation. Ipilimumab (Yervoy) blocks CTLA-4, boosting the overall T-cell response.
Recent trial results highlight just how powerful these drugs have become. In the KEYNOTE-689 trial (published in NEJM 2025), adding pembrolizumab to standard treatment for locally advanced head and neck cancer improved 3-year event-free survival to 59.8% compared to 45.9% with standard care alone, a clinically meaningful improvement.
CAR-T Cell Therapy
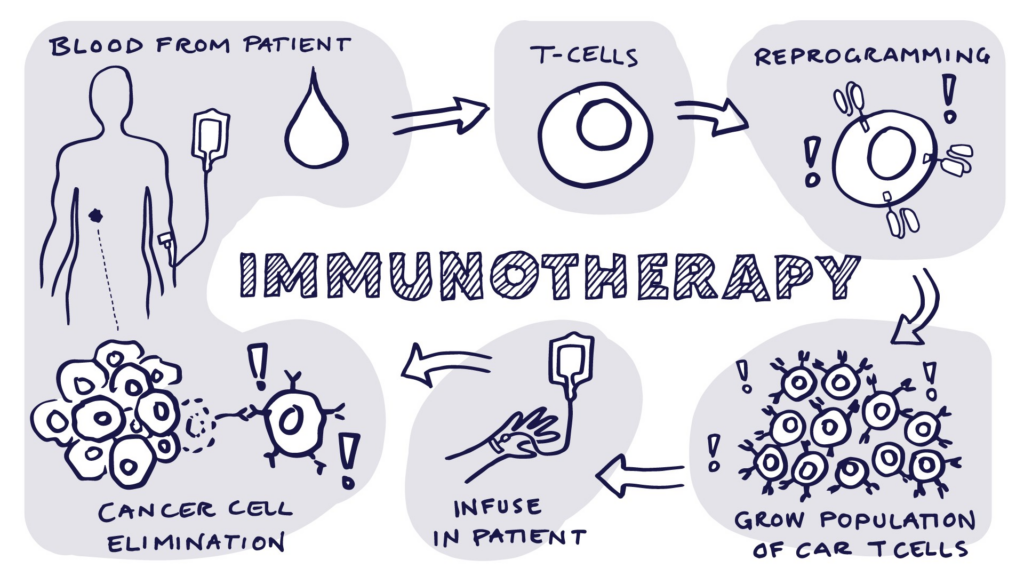
CAR-T cell therapy (Chimeric Antigen Receptor T-cell therapy) is one of the most personalized cancer treatments ever developed. It involves:
- Extracting T-cells from the patient’s own blood
- Genetically engineering those cells in a laboratory to carry a special receptor (CAR) that specifically recognizes proteins on the cancer cells
- Growing millions of these engineered cells
- Infusing them back into the patient, where they seek out and destroy cancer cells
CAR-T therapy has shown particularly remarkable results in blood cancers, including certain types of leukemia and lymphoma, with some patients experiencing complete remissions after all other treatments had failed. The approach is increasingly being explored for solid tumors, though this remains more challenging. See our post on gene therapy and blood disorders for related context on how genetic engineering is reshaping medicine.
Cancer Vaccines
Unlike the vaccines you receive to prevent infectious diseases, therapeutic cancer vaccines are designed to treat existing cancer by teaching the immune system to recognize cancer-specific proteins and mount an attack.
The mRNA vaccine technology that gained global attention during the COVID-19 pandemic is now being applied to cancer. A landmark study found that mRNA-4157 (a personalized cancer vaccine) combined with pembrolizumab reduced melanoma recurrence risk by 44% compared to checkpoint inhibitor therapy alone, a result published in 2025 that has energized the field. Over 120 clinical trials for mRNA-based cancer vaccines were underway as of 2025, with promising early results in pancreatic cancer and brain tumors.
Monoclonal Antibodies
Monoclonal antibodies are lab-engineered proteins designed to recognize and bind to specific targets on cancer cells or on immune cells. They can work in several ways: by flagging cancer cells for destruction, delivering toxic payloads directly to tumors (antibody-drug conjugates), or blocking growth signals. Trastuzumab (Herceptin) and cetuximab are examples you may have heard of.
Cytokines
Cytokines (such as interleukins and interferons) are naturally occurring signaling proteins that the immune system uses to coordinate its response. Synthetic versions can be administered to amplify immune activity against cancer, though these therapies tend to have significant side effects and are used in more specific contexts.
What Does the Evidence Actually Show?
Immunotherapy’s track record is genuinely impressive, but it’s also important to be precise about what it achieves and for whom.
Where Immunotherapy Has Been Transformative
The clearest wins have been in cancers where checkpoint inhibitors have converted once-dire diagnoses into manageable or even curable disease:
- Melanoma, Advanced melanoma once had a median survival of less than a year. With combination checkpoint blockade (anti-PD-1 + anti-CTLA-4), a significant proportion of patients now achieve long-term remission. Some trials now report 10-year survival rates above 20% for a disease that was once almost universally fatal at advanced stages.
- Non-small cell lung cancer (NSCLC), Pembrolizumab has transformed treatment for patients with high PD-L1 expression, with 5-year survival rates in some subgroups exceeding 20–30% compared to less than 5% historically with chemotherapy alone.
- Bladder cancer, A 2024 trial (Niagara Trial) showed that adding immunotherapy to treatment reduced the risk of recurrence by 32% and the risk of death by 25% compared to chemotherapy alone.
- Head and neck cancers, As noted above, checkpoint inhibitors have improved outcomes significantly for recurrent or locally advanced disease.
Where the Picture Is More Complex
Not everyone responds to immunotherapy, and this is one of the field’s most important active research questions. Response rates to checkpoint inhibitors alone range from around 20–40% in many cancers. Researchers are working intensively to identify biomarkers, biological signals, that can predict who is likely to respond, so that treatment can be better matched to patient.
Factors that currently influence likelihood of response include PD-L1 expression on the tumor, tumor mutational burden (TMB) (how many genetic mutations the cancer carries, higher can mean more visible to the immune system), and the specific genetic characteristics of the cancer.
Combining immunotherapy with chemotherapy, radiation, or targeted therapies, so-called combination strategies, has consistently shown better results than any single approach alone and represents the dominant direction of current research. The incorporation of immune checkpoint inhibitors into the treatment of non-small cell lung cancer has improved outcomes across early-stage, locally advanced, and metastatic settings.
Side Effects: What Immunotherapy Can Do to Your Body
Immunotherapy is often described as better-tolerated than chemotherapy, and in many ways it is. But that doesn’t mean it’s without side effects. Because immunotherapy amplifies the immune system’s activity broadly, it can sometimes cause inflammation in healthy tissues and organs, a category of side effects called immune-related adverse events (irAEs).
Common Side Effects
- Fatigue, One of the most frequently reported effects across all immunotherapy types
- Skin reactions, Rashes, itching, and dermatitis are among the most common; generally manageable
- Diarrhea and colitis, Inflammation of the gut lining is a frequent irAE
- Nausea and appetite loss
- Flu-like symptoms, Particularly with cytokine-based therapies
Serious but Less Common Side Effects
In a small proportion of patients, the immune system can attack major organs, causing more serious complications:
- Pneumonitis (lung inflammation)
- Hepatitis (liver inflammation)
- Endocrinopathies, Thyroid, adrenal, or pituitary gland dysfunction; sometimes permanent
- Myocarditis (heart inflammation), Rare but potentially life-threatening; an area of active cardio-oncology research as of 2025
These serious events are more common with combination checkpoint blockade (using two checkpoint inhibitors together) than with single-agent therapy. Treatment is typically paused and corticosteroids are administered for grade 2 or higher toxicities. Most side effects resolve with appropriate management, but some, particularly endocrine effects, can be long-lasting.
CAR-T Specific Side Effects
CAR-T cell therapy carries its own distinct risk profile, including:
- Cytokine Release Syndrome (CRS), A potentially severe inflammatory reaction caused by the rapid activation of large numbers of immune cells; manageable in most patients but serious in some
- Neurotoxicity, A neurological syndrome that can cause confusion, difficulty speaking, or seizures in some patients; usually reversible
Management of these side effects requires specialist care at experienced centers.
Immunotherapy vs. Chemotherapy: What’s the Difference?
A common question people have is how immunotherapy differs from chemotherapy. The short answer is: fundamentally.
Chemotherapy works by targeting rapidly dividing cells, which includes cancer cells, but also includes hair follicle cells, gut lining cells, and bone marrow cells. This is why chemotherapy causes hair loss, nausea, and immune suppression. It attacks cancer directly but collaterally damages healthy tissue.
Immunotherapy doesn’t directly attack cells at all. It modifies the immune system’s behavior, either removing brakes, adding new weapons, or teaching it what to target. Side effects arise from immune overactivation rather than direct tissue damage.
In practice, these two approaches are increasingly used together. Combining immunotherapy with chemotherapy often yields better outcomes than either alone, because chemotherapy can destroy cancer cells in ways that make them more visible to the newly-activated immune system.
Who Is Immunotherapy Right For?
Immunotherapy is not a universal treatment. Whether it’s appropriate for a particular patient depends on several factors:
- Cancer type and stage, Some cancers respond much better than others; your oncologist will know which immunotherapy options are approved or in trials for your specific diagnosis
- Tumor biomarkers, PD-L1 expression, TMB, and other markers are increasingly used to predict response
- Overall health and immune function, Active autoimmune diseases can be a contraindication to certain immunotherapies, as amplifying the immune system could worsen autoimmune conditions
- Previous treatments, Some immunotherapies are approved as first-line treatment; others are reserved for cancers that have progressed after other therapies
- Access to specialized centers, CAR-T therapy, in particular, is currently available only at designated treatment centers
The most important step is a detailed conversation with an oncologist who specializes in your cancer type. A tumor biomarker test (often done on a biopsy sample) can help identify whether immunotherapy is likely to be effective.
The Future of Immunotherapy: Where Research Is Heading
The pace of immunotherapy research is extraordinary. Here are some of the most exciting directions as of 2026:
Personalized Cancer Vaccines
Building on the mRNA technology platform, personalized neoantigen vaccines, custom-designed to match the unique mutation profile of an individual patient’s tumor, represent potentially the most precise cancer treatment ever conceived. The 44% reduction in melanoma recurrence seen with the mRNA-4157 + pembrolizumab combination in 2025 has accelerated investment and trials in this space across many cancer types.
Bispecific Antibodies
Bispecific antibodies are engineered to simultaneously bind to a cancer cell and to a T-cell, physically bringing them together to trigger destruction. Multiple bispecific antibodies are now approved for blood cancers, and the technology is being rapidly extended to solid tumors.
Overcoming Resistance
A central challenge of current immunotherapy is that many patients who initially respond eventually develop resistance, and the cancer finds new ways to evade the immune system. Research into resistance mechanisms, and into treatment strategies (including novel combinations) to overcome them, is one of the most active areas in oncology.
Beyond Cancer
It’s worth noting that immunotherapy applications extend beyond oncology. Allergy immunotherapy (allergy shots) is an established, decades-old practice for desensitizing the immune system to allergens. Research is also exploring immunotherapy approaches for autoimmune diseases, infectious diseases, and even neurodegenerative conditions.
Key Takeaways
- Immunotherapy works by harnessing and enhancing the body’s own immune system to fight cancer, rather than directly attacking tumor cells, a fundamentally different approach from chemotherapy and radiation.
- The main types include checkpoint inhibitors (the most widely used), CAR-T cell therapy, cancer vaccines (including mRNA-based), monoclonal antibodies, and cytokines, each with distinct mechanisms and use cases.
- Results have been transformative for certain cancers, particularly advanced melanoma, lung cancer, bladder cancer, and some head and neck cancers, with survival rates improving dramatically over the past decade.
- Not everyone responds to immunotherapy; biomarkers like PD-L1 expression and tumor mutational burden help predict who is most likely to benefit, and combination approaches are increasingly the standard.
- Side effects are different from, not necessarily milder than, chemotherapy; immune-related adverse events can affect any organ system and require prompt medical management.
Closing: A Genuine Revolution, With Important Nuance
Immunotherapy represents one of the most significant advances in medicine in a generation. For many patients with cancers that were once considered incurable, it has offered something that felt impossible a decade ago: genuine hope. The science continues to move fast, with personalized vaccines, novel combinations, and next-generation CAR-T therapies reshaping what’s achievable year by year.
But it’s also a field where nuance matters. Immunotherapy isn’t right for everyone, isn’t effective against every cancer, and comes with its own set of side effects that require careful management. The best outcomes come from an experienced, multidisciplinary oncology team that can assess your specific situation using the latest biomarker data and clinical evidence.
If you or someone you know is navigating a cancer diagnosis, ask your oncologist specifically whether immunotherapy, or a clinical trial involving immunotherapy, might be an option. It’s a question worth asking. And if you’d like to learn more about specific cancers where immunotherapy is already making a major difference, explore our related posts on tonsil cancer treatment and sickle cell disease and gene therapy.