A critical investigation into why BIPOC women face dangerous delays and denials for cancer biopsies, creating life-threatening diagnostic disparities. Learn the systemic causes and vital solutions.
Introduction
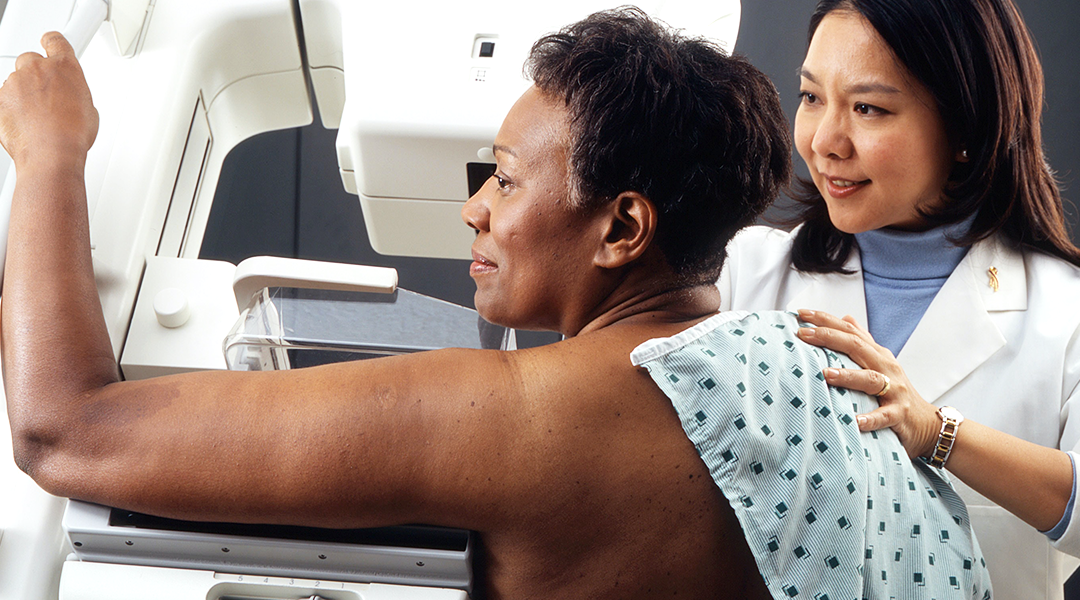
A cancer biopsy is more than a medical procedure; it is a critical gateway. A timely biopsy can mean the difference between a Stage I and a Stage IV diagnosis, between a treatable condition and a terminal one. For far too many Black, Indigenous, and People of Color (BIPOC) women in the United States, this gateway is blocked by a complex web of barriers, leading to a devastating reality: they are more likely to be diagnosed with advanced cancer and more likely to die from it.
This article moves beyond acknowledging this tragic statistic to dissect the “why” behind it. We will examine how systemic failures—from insurance chasms and provider bias to geographic deserts and cultural distrust—converge to create a deadly bottleneck at the point of diagnosis. This is not merely a healthcare gap; it is a biopsy crisis with mortal consequences.
The Stark Reality: A Tale of Two Outcomes
The data paints an unambiguous and alarming picture. According to the American Cancer Society, Black women have a 40% higher death rate from breast cancer than white women, despite a slightly lower incidence rate. They are twice as likely to die from endometrial cancer. Native American and Alaskan Native women have the highest cervical cancer death rates of any racial/ethnic group.
These disparities are not primarily due to biological differences. They are the direct result of being diagnosed at a later, less treatable stage. The bottleneck occurs before treatment even begins, in the crucial phases of symptom recognition, referral, and diagnostic biopsy.
Deconstructing the Barriers: Why the Biopsy Bottleneck Exists
The pathway to a biopsy is fraught with systemic obstacles that disproportionately affect BIPOC women.
1. The Referral Gap: When Symptoms Are Dismissed
The journey often halts at the primary care office. Implicit bias significantly impacts clinical decision-making. Studies consistently show that pain and symptoms reported by Black patients are taken less seriously. Abnormal bleeding, a persistent cough, or a palpable lump may be attributed to benign causes for longer periods, delaying specialist referral. The “watchful waiting” approach is applied more frequently to women of color, during which time a curable cancer can progress.
2. The Insurance Abyss: The Cost of a Diagnosis
Even with a referral, the financial barrier is immense. BIPOC women are more likely to be underinsured or rely on Medicaid, which often has lower reimbursement rates for procedures. Some specialists may be reluctant to schedule a biopsy for patients with these plans. High deductibles and co-pays can make the biopsy itself financially catastrophic, forcing patients to choose between a diagnosis and other essential needs like rent or groceries.
3. The Geographic Desert: No Specialist in Sight
Geographic disparities in healthcare access are profound. Many predominantly BIPOC communities are “specialty deserts,” with few or no oncologists or surgical specialists within a reasonable distance. Getting a biopsy may require taking multiple days off work, securing childcare, and arranging long-distance travel—an insurmountable hurdle for many.
4. The Trust Deficit: A Legacy of Harm
Historical and ongoing medical exploitation, like the Tuskegee Syphilis Study, has bred a deep and justified distrust of the medical system among many BIPOC communities. This distrust can make women hesitant to pursue aggressive diagnostic steps, especially if they feel their concerns were previously dismissed. The lack of racial concordance in oncology—where fewer than 3% of practicing oncologists are Black—can further exacerbate this communication and trust gap.
The Human Cost: Beyond Statistics
The consequence of these delays is measured in human lives. A later-stage diagnosis means more aggressive, more debilitating, and more expensive treatments with lower success rates. It means families losing mothers, daughters, and sisters to cancers that could have been cured. It perpetuates a cycle of fear and mistrust, validating the very concerns that the system fails to address.
Forging Solutions: A Multifaceted Path to Equity
Solving this crisis requires dismantling barriers at every level.

For the Healthcare System:
- Mandatory Implicit Bias Training: This must move from elective seminars to accredited, mandatory training for all clinical staff, with accountability measures.
- Standardized Diagnostic Pathways: Implementing clear, symptom-based clinical protocols for specialist referral can help remove subjective bias from the decision to biopsy.
- Invest in Community Care: Funding must be directed to clinics and hospitals serving BIPOC communities, ensuring they have the resources and specialist partnerships to perform biopsies on-site.
For Providers:
- Practice Culturally Competent, Patient-Centered Care: Listen actively. Believe the patient. Use tools like the CDC’s “My Family Health Portrait” to formally assess risk. Explain the “why” behind every decision, especially when not pursuing a biopsy.
- Build a Referral Network that Accepts All Insurance: Proactively create pathways for uninsured and publicly insured patients to receive timely diagnostics.
For Patients and Advocates:
- Empowerment Through Preparation: Document symptoms meticulously. Know your family history. Use clear, direct language to advocate for your care (“My understanding is that these symptoms warrant a biopsy. Can you explain why we are choosing a different path?”).
- Utilize Patient Navigators: Many hospitals have navigators who can help guide you through financial assistance, scheduling, and transportation for procedures.
- Seek Second Opinions Unapologetically: If you feel your concerns are being minimized, a second opinion is not a sign of disrespect; it is a standard of good care.
Conclusion: A Matter of Justice and Survival
The disparity in cancer biopsy access for BIPOC women is not a niche healthcare issue; it is a glaring indicator of systemic failure and a matter of life and death. It reveals how racism and inequality are embedded in the very architecture of medicine, from the doctor’s office to the insurance ledger.
Closing this gap requires more than awareness. It demands a fundamental restructuring of priorities, funding, and clinical practice to ensure that the gateway to diagnosis—and thus, to survival—is equally open to all. The goal is unambiguous: a woman’s zip code, insurance card, or skin color should never determine the stage at which her cancer is found. Achieving equity in the biopsy room is the first, non-negotiable step toward achieving equity in cancer survival.
FAQs
Q1: What are the most common cancers where BIPOC women face biopsy and diagnostic delays?
A1: Disparities are stark in breast, cervical, endometrial, and colorectal cancers. For example, Black women are more likely to be diagnosed with later-stage breast cancer and more aggressive subtypes, partly due to delays in imaging follow-up and biopsy access. They are also twice as likely to die from endometrial cancer, often after reporting symptoms like abnormal bleeding for longer periods before a diagnostic biopsy is performed.
Q2: Is the main issue that doctors are overtly racist?
A2: Overt discrimination exists, but the larger, more pervasive issue is implicit bias—unconscious stereotypes that affect clinical judgment. Studies show that pain and symptoms reported by Black patients are systematically underrated. A physician’s unconscious bias can lead to dismissing concerning symptoms as “stress” or “weight-related,” opting for “watchful waiting” instead of an immediate diagnostic biopsy for a patient of color, while recommending the biopsy for a white patient with identical symptoms.
Q3: As a BIPOC woman, what can I do if I feel my symptoms are being dismissed?
A3: Empowerment is key. Come prepared: document your symptoms and family history clearly. Use direct language: “I am concerned about cancer. What are the criteria for a biopsy, and do my symptoms meet them?” Ask for a denial to be noted in your chart. Seek a second opinion without hesitation. Bring a trusted advocate to appointments. You are the expert on your own body.