If you’ve had unexplained, watery diarrhea that just won’t quit this summer, you’re not imagining things, and you’re not alone. As of mid-June 2026, health officials had confirmed at least 145 domestically acquired cases of cyclosporiasis across 17 states, with a fast-growing cluster in southeast Michigan pushing case counts even higher in the weeks since. The source of the current outbreak still hasn’t been pinned down.
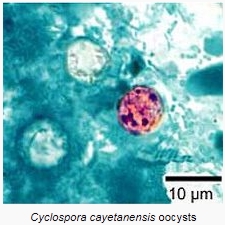
The parasite behind it all is called Cyclospora cayetanensis, and it’s easy to miss. Standard stool tests don’t screen for it, so a lot of people spend weeks feeling awful, assuming they have a stubborn stomach virus, when a very treatable parasitic infection is actually to blame.
This post breaks down what Cyclospora is, how you catch it, what the current outbreak looks like, and, most importantly, what to say to your doctor if you suspect you have it.
What Is Cyclospora, and How Do You Get It?
Cyclospora is a microscopic, single-celled parasite that causes an intestinal illness called cyclosporiasis. It spreads through the fecal-oral route, meaning infection happens when you eat food or drink water contaminated with feces containing the parasite.
Here’s a detail that surprises a lot of people: you can’t catch Cyclospora directly from another sick person. After the parasite is shed in stool, it needs to spend one to several weeks in the environment before it becomes infectious, a process called sporulation. That built-in delay is why person-to-person spread is considered highly unlikely.
In the United States, past outbreaks have consistently been traced back to imported and domestic fresh produce, especially cilantro, basil, raspberries, snow peas, and bagged salad mixes. The parasite is more common in tropical and subtropical regions, so international travel has historically been a major risk factor, but a growing share of U.S. cases now have no travel history at all and are linked to food eaten right here at home.
The 2026 Outbreak: What We Know So Far
This isn’t a one-off event, Cyclospora has an established seasonal pattern in the U.S., with the “cyclosporiasis season” officially running from May 1 through August 31 each year. But 2026 stands out for its scale and the fact that investigators still haven’t found the source.
According to CDC surveillance data, 145 domestically acquired cases had been reported across 17 states as of June 16, 2026, with 20 people hospitalized and no deaths. An additional 45 cases were linked to international travel, with 3 hospitalizations among that group. New York has reported the highest concentration of cases so far.
Since then, the picture has shifted further: southeast Michigan alone reported more than 170 cases by late June, a dramatic jump for a state that typically sees only about 50 cases in an entire year. That local spike has expanded into at least seven counties, and health officials there are actively investigating the cause.
For context, this isn’t unprecedented in scale, 2025 was itself a heavy year, with 1,180 domestically acquired cases reported across 38 states. What’s different in 2026 is that, weeks into the investigation, the FDA and CDC still haven’t identified a specific food source, which reflects how difficult traceback can be for fresh produce that moves through complex, often global supply chains.
Recognizing the Symptoms
Cyclosporiasis has a fairly distinctive symptom profile, even though it’s frequently mistaken for a stomach bug. Symptoms typically appear two to 14 days after exposure, and can include:
- Frequent, watery diarrhea, often described as “explosive”
- Loss of appetite
- Abdominal cramping and bloating
- Nausea (vomiting is less common)
- Fatigue
- Low-grade fever
- Weight loss over time
One of the most telling features of this illness is its relapsing pattern. Left untreated, symptoms can last anywhere from a few days to over a month, and they often seem to improve before suddenly returning. If your “stomach bug” has already come back once after you thought it was over, that’s a meaningful clue worth mentioning to your doctor.
Why Cyclospora Gets Missed So Often
Here’s the part that frustrates a lot of patients after the fact: routine stool cultures do not test for Cyclospora. Unless a physician specifically orders testing for it, usually through modified acid-fast staining or PCR-based testing, the infection can go completely undiagnosed.
This means many people who assume they had a “three-week virus” actually had a treatable parasitic infection the whole time. Health officials note that confirmed case counts, including the 145 cases reported in the current outbreak, likely represent a significant undercount of the true number of infections, precisely because testing isn’t automatic.
If you develop watery diarrhea lasting more than five days, especially during the summer months, and especially if it follows a pattern of improving and then relapsing, it’s worth asking your healthcare provider directly whether Cyclospora testing makes sense, rather than waiting for it to be offered by default.
[link to post on food safety and produce washing
Diagnosis and Treatment
If Cyclospora is suspected, your doctor can order a stool test using specialized methods (acid-fast staining or PCR) rather than a standard culture. Because the parasite is shed intermittently, sometimes more than one stool sample is needed to catch it.
The standard treatment is a combination antibiotic called trimethoprim-sulfamethoxazole, commonly known by the brand name Bactrim, and it’s generally very effective. Most healthy people who receive appropriate treatment recover fully.
There currently isn’t a well-established alternative for people who can’t tolerate sulfa drugs due to allergy; in those cases, your provider may recommend supportive care (staying hydrated and managing symptoms) or a referral to an infectious disease specialist.
People with weakened immune systems, including those with HIV/AIDS or who are on immunosuppressive medications, are at higher risk of prolonged illness, more severe symptoms, and relapse, and should be monitored closely by their care team.
Notably, most people with healthy immune systems will eventually clear the infection on their own even without treatment, though getting properly diagnosed and treated significantly shortens the misery and reduces the risk of relapse.
How to Lower Your Risk
Since Cyclospora is tied so closely to contaminated fresh produce and water, prevention comes down to a few practical habits:
- Wash all fresh produce, including pre-washed and bagged salad greens, under cold running water before eating. This reduces, but doesn’t fully eliminate, contamination, since Cyclospora oocysts are resistant to many common disinfectants.
- Be cautious with unfiltered or untreated water, particularly when traveling in regions where cyclosporiasis is more common.
- Stay informed about active outbreak advisories in your area, especially during peak season (May through August), and check for any product recalls linked to fresh herbs or produce.
- Practice good hand hygiene, especially after using the bathroom and before preparing food, to avoid contributing to fecal-oral spread.
No method of washing produce guarantees complete removal of the parasite, which is part of why traceback investigations focus heavily on stopping contaminated products at the source rather than relying on consumers alone.
Key Takeaways
- Cyclospora cayetanensis causes a relapsing, watery diarrheal illness that’s easy to mistake for a routine stomach virus.
- A significant 2026 outbreak is ongoing, with 145+ domestically acquired cases across 17 states as of mid-June, plus a fast-growing cluster in Michigan, the source hasn’t yet been identified.
- Routine stool tests don’t screen for Cyclospora, if your diarrhea lasts more than five days or keeps coming back, specifically ask your doctor to test for it.
- Treatment with trimethoprim-sulfamethoxazole (Bactrim) is highly effective; most people recover fully once properly diagnosed.
- Wash fresh produce thoroughly, stay alert to outbreak advisories during peak season (May–August), and don’t assume a lingering summer stomach bug is “just a virus.”
The Bottom Line
Cyclospora is a good example of how an infection can be both common and consistently under-recognized, not because it’s mysterious, but because it simply isn’t part of standard testing. If you’ve had watery, relapsing diarrhea this summer that’s stuck around longer than a typical stomach bug, don’t just wait it out.
Talk to your healthcare provider, describe the pattern of your symptoms clearly, and ask specifically about Cyclospora testing. It’s a simple conversation that can turn weeks of guessing into a clear diagnosis and an effective, short course of treatment.