Introduction
Most people think of chickenpox as a childhood rite of passage, a week of itchy spots, followed by a lifetime of immunity. And for most people, that’s the whole story. But the virus responsible, the varicella zoster virus (VZV), never fully leaves your body. It retreats into nerve cells near your spine and skull, where it can lie dormant for decades. When it reactivates, it causes shingles. And in some cases, it does something far more dangerous: it invades the brain.
VZV-related brain inflammation, encompassing encephalitis (inflammation of the brain tissue itself) and vasculopathy (inflammation of the blood vessels supplying the brain, which can cause stroke), is a serious but underdiagnosed neurological condition. It is estimated to cause 5–8% of all adult encephalitis cases, according to Neurology Neuroimmunology & Neuroinflammation. And critically, it can occur without the classic shingles rash, making it easy to miss. A 2025 case series published in Frontiers in Neurology reviewed 108 non-immunocompromised patients with VZV central nervous system infection, illustrating that even otherwise healthy people can be affected.
In this post we explain what VZV brain inflammation is, how it develops, who is at risk, what warning signs to look for, how it is diagnosed and treated, and, most importantly, how vaccination can protect you. This is a topic that deserves more public awareness than it gets.
→ Related: link to immunotherapy and the immune system
UNDERSTANDING THE VARICELLA ZOSTER VIRUS
To understand VZV brain inflammation, you first need to understand the virus’s two-act life cycle.
Act One, Chickenpox (Varicella)
Varicella zoster virus (VZV) is a member of the herpesvirus family. During its primary infection, chickenpox, VZV spreads across the skin and mucous membranes, causing the familiar itchy blister rash. Most people encounter it in childhood. The infection resolves within 1–2 weeks, and the immune system contains the virus. But containment is not elimination.
After primary infection, VZV travels along sensory nerve pathways to dorsal root ganglia, clusters of nerve cell bodies that run along the spine, and to cranial nerve ganglia in the head and neck. There it becomes latent: silent, invisible on routine tests, and protected from the immune system inside nerve cells. It can remain there for the rest of a person’s life without causing further problems.
Act Two, Shingles (Herpes Zoster) and Neurological Complications
Decades later, typically when the immune system weakens with age, illness, or medication, VZV can reactivate. The reactivated virus travels back along the nerve fibres, causing the painful blistering rash of shingles (herpes zoster), usually appearing on one side of the body or face.
But reactivation doesn’t always stay neatly within the skin and its supplying nerves. In some cases, VZV spreads into the central nervous system (CNS), the brain and spinal cord, where it can cause a spectrum of serious complications, including:
- Encephalitis, inflammation of brain tissue
- Meningitis, inflammation of the protective membranes (meninges) surrounding the brain
- Myelitis, inflammation of the spinal cord
- Vasculopathy, inflammation of the arteries supplying the brain, which can lead to stroke
- Cranial nerve palsies, including facial palsy and ophthalmic complications (Ramsay Hunt Syndrome)
According to Encephalitis International (2025), VZV encephalitis has an estimated incidence of 1–2 cases per 10,000 varicella infections. While that sounds rare, given how common chickenpox exposure is globally, this translates to significant real-world case numbers.
TWO DISTINCT SYNDROMES: ENCEPHALITIS VS. VASCULOPATHY
It’s important to distinguish between the two main ways VZV can affect the brain, because they present differently, carry different risks, and require slightly different approaches to management.
VZV Encephalitis
In VZV encephalitis, the virus directly infects and inflames brain tissue. The result is a combination of:
• Fever
• Headache (often severe)
• Confusion, disorientation, or altered consciousness
• Seizures
• Focal neurological deficits (weakness, speech problems, visual changes, depending on which part of the brain is affected)
A 2025 study in Frontiers in Neurology examining 108 non-immunocompromised patients with VZV CNS infection found that the most commonly affected brain regions were the parietal lobe, followed by the frontal and temporal lobes. The study highlighted that lesions can present as ischemic stroke, intracerebral haemorrhage, or venous sinus thrombosis.
CRITICAL ALERT: RASH-FREE PRESENTATION
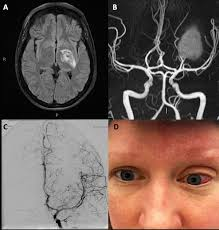
VZV encephalitis can, and frequently does, occur WITHOUT the characteristic shingles rash. This “zoster sine herpete” (shingles without rash) presentation is a major cause of delayed diagnosis. A 2025 case report described VZV encephalitis so closely mimicking a brain tumour (glioblastoma) on MRI that antiviral treatment was delayed, worsening outcomes.
VZV Vasculopathy, The Hidden Stroke Risk
VZV vasculopathy is described in a 2024 review in Cureus as a “rare yet potentially severe neurological manifestation” that remains severely underdiagnosed. Here, VZV infects the walls of arteries supplying the brain, causing inflammation, thickening of the artery lining (intima), and loss of smooth muscle cells. The consequences include:
• Ischemic stroke, the most common outcome, caused by vessel narrowing or clot formation
• Haemorrhagic stroke, vessel rupture causing bleeding into the brain
• Venous sinus thrombosis, blood clots in the veins draining the brain
VZV vasculopathy can affect both large cerebral arteries (causing major strokes) and small deep vessels (causing white matter lesions). A 2025 Frontiers in Medicine case report described a child developing intracranial haemorrhagic vasculitis from VZV, illustrating that this complication is not confined to adults.
Crucially, VZV vasculopathy can occur weeks to months after shingles, with the rash long resolved. The neurological event may seem entirely unrelated to the prior shingles episode, another reason it is chronically underdiagnosed.
WHO IS AT RISK?
VZV brain complications can affect anyone who has previously had chickenpox, which includes virtually the entire pre-vaccine adult population worldwide. However, several factors significantly elevate risk.
Immune Status
The most important risk factor is weakened cell-mediated immunity, the arm of the immune system responsible for keeping latent VZV in check. Risk is elevated in:
- Older adults, immune function naturally declines with age; VZV reactivation risk doubles approximately every decade after age 50
- HIV/AIDS, VZV encephalitis carries an estimated 33% mortality in HIV-infected patients with catastrophic outcomes even when treated
- Solid organ or bone marrow transplant recipients, a 2025 analysis found 33% of allogenic haematopoietic stem cell transplant recipients experienced VZV reactivation
- People on long-term immunosuppressant medications, including corticosteroids, chemotherapy, biologic treatments (e.g. for rheumatoid arthritis or IBD), and others
- People with blood cancers (leukaemia, lymphoma)
Other Risk Factors
- Herpes zoster ophthalmicus (HZO), shingles affecting the eye branch of the trigeminal nerve is particularly associated with VZV vasculopathy, because of the anatomical proximity of these nerve pathways to cerebral vessels
- Ramsay Hunt Syndrome, a 2025 Frontiers in Neurology review specifically identified this as a trigger for VZV vasculopathy
- Prior chickenpox without vaccination, natural infection establishes stronger latency than vaccinated immunity in some analyses
Important caveat: as the 2025 Frontiers in Neurology cohort study of 108 patients demonstrates, VZV CNS complications do occur in non-immunocompromised (otherwise healthy) individuals. Immune deficiency greatly amplifies risk but is not a requirement.
SYMPTOMS, WHAT TO WATCH FOR
VZV brain inflammation has no single “signature” presentation. Symptoms vary based on whether the predominant process is encephalitis, vasculopathy, meningitis, or a combination. The timeline also varies: symptoms can begin during an active shingles episode or appear weeks to months after apparent recovery.
Warning Signs of VZV Encephalitis
◆ Severe or persistent headache, especially new, unlike prior headaches
◆ High fever
◆ Confusion, disorientation, or altered behaviour
◆ Drowsiness or reduced consciousness
◆ Seizures (new onset)
◆ Sensitivity to light (photophobia) or sound
◆ Neck stiffness (suggesting meningeal involvement)
◆ Speech difficulties or slurred speech
◆ Weakness or numbness on one side of the body
◆ Visual disturbances
Warning Signs of VZV Vasculopathy (Stroke)
VZV vasculopathy should be considered in any person who develops stroke-like symptoms, particularly weeks to months after a shingles episode. The classic FAST stroke warning signs apply:
◆ F, Face drooping (sudden, one-sided)
◆ A, Arm weakness (sudden, one-sided)
◆ S, Speech difficulty (sudden slurring or inability to speak or understand)
◆ T, Time to call emergency services immediately
EMERGENCY WARNING
Any of these symptoms, whether or not you have a rash, constitute a medical emergency. Call your local emergency services immediately. Do not drive yourself to the hospital. Do not wait to see if symptoms improve overnight.
DIAGNOSIS, HOW DOCTORS IDENTIFY VZV BRAIN INFLAMMATION
Diagnosing VZV CNS complications requires a combination of clinical assessment, imaging, and laboratory tests. It is notoriously challenging, particularly when the characteristic rash is absent, which is why clinical suspicion matters enormously.
Lumbar Puncture and CSF Analysis
The cornerstone diagnostic test is a lumbar puncture (spinal tap) to obtain cerebrospinal fluid (CSF), the fluid surrounding the brain and spinal cord. Key CSF findings in VZV CNS disease:
- VZV DNA by PCR (polymerase chain reaction), the gold standard for detecting active VZV infection in the CNS; highly specific. PCR can detect VZV DNA rapidly, per CDC 2024 guidance.
- VZV-specific IgG antibodies in CSF, can be positive even when PCR is negative, and may be more sensitive in certain phases of the illness
- Elevated white blood cell count (pleocytosis), indicating CNS inflammation
- Elevated protein levels
Note: CSF PCR for VZV can be negative in up to 40% of VZV vasculopathy cases, which is why combined PCR plus antibody testing is recommended when VZV CNS disease is suspected.
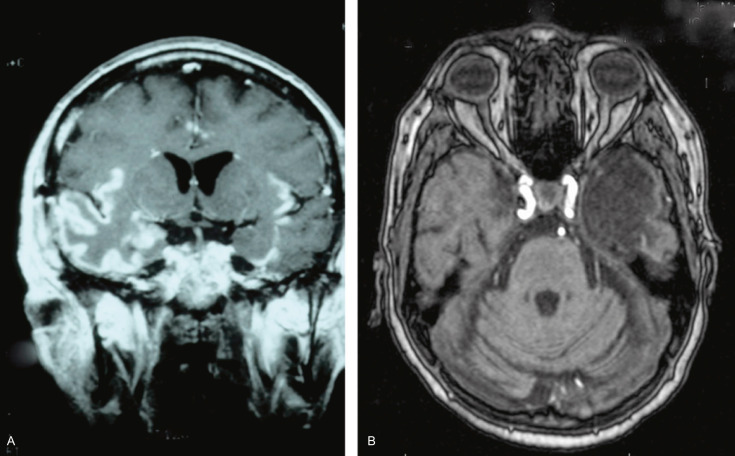
Brain Imaging
• MRI (magnetic resonance imaging), the primary imaging modality; can reveal areas of infarction, haemorrhage, white matter lesions, or vessel wall enhancement. However, as a 2025 case report highlighted, MRI appearances can occasionally mimic brain tumours, leading to diagnostic delay.
• MRI angiography (MRA) or CT angiography (CTA), assess the cerebral blood vessels for vasculopathy changes: narrowing, irregularity, or vessel wall thickening and enhancement.
• EEG (electroencephalogram), measures brain electrical activity; can detect seizure activity and patterns associated with encephalitis.
The Diagnostic Challenge
VZV vasculopathy is described by Cureus (2024) as “an underdiagnosed condition.” Reasons include:
• Rash may be absent or have resolved weeks earlier
• CSF PCR can be falsely negative
• MRI findings can be non-specific
• Neurologists may not immediately associate a stroke with a prior shingles episode
A high index of clinical suspicion, particularly in older, immunocompromised, or post-shingles patients, is essential for timely diagnosis.
TREATMENT, SPEED MATTERS ENORMOUSLY
Early treatment is the single most important factor in improving outcomes for VZV brain inflammation.
Intravenous Acyclovir, The Mainstay
Intravenous (IV) acyclovir is the first-line antiviral treatment for VZV CNS complications. It works by blocking the VZV enzyme (thymidine kinase) required for viral DNA replication, halting the spread of active infection. Key points:
• Standard treatment course: 10–14 days of IV acyclovir for CNS disease (longer than for uncomplicated shingles)
• Treatment should be initiated as soon as VZV CNS disease is clinically suspected, ideally without waiting for laboratory confirmation, given the urgency
• Per Encephalitis International (2025), early acyclovir administration reduces severity and duration of illness
• For acyclovir-resistant VZV (primarily a concern in severely immunocompromised patients), foscarnet is used as an alternative
Corticosteroids, A Considered Addition
In VZV vasculopathy, the arterial damage is driven partly by inflammation rather than active viral replication alone. This is why the 2024 Cureus case series described treating patients with a combination of IV acyclovir plus oral prednisolone, the corticosteroid helps dampen the inflammatory component of vessel wall disease.
A case of VZV haemorrhagic encephalitis with vasculopathy reported in Neurology Neuroimmunology & Neuroinflammation was treated with foscarnet (for acyclovir resistance) and IV methylprednisolone.
The use of corticosteroids in VZV CNS disease is not universally standardised, decisions are made on a case-by-case basis in consultation with neurology and infectious disease specialists.
Supportive Care
Beyond antivirals, patients with VZV encephalitis require intensive supportive care:
• Seizure management (anti-epileptic medications as needed)
• Fever control
• IV fluids for hydration
• Stroke management protocols for vasculopathy (including anticoagulation or antiplatelet therapy where indicated)
• Neurological monitoring in an intensive or specialist setting
Per Medscape (2026), neurology and infectious disease specialist consultations are both indicated for confirmed or suspected VZV encephalitis or myelitis.
OUTCOMES AND LONG-TERM EFFECTS
Outcomes of VZV brain inflammation vary widely, depending on the syndrome (encephalitis vs. vasculopathy), severity at presentation, and how quickly treatment is started.
• Complete recovery is possible, particularly with early treatment in otherwise healthy individuals
• Neurological sequelae, including memory problems, cognitive impairment, weakness, speech difficulty, and epilepsy, are common after severe disease
• Mortality, VZV encephalitis carries meaningful mortality risk. In HIV-infected patients, mortality is estimated at around 33%. In non-immunocompromised adults, mortality is lower but still significant in severe cases.
• Stroke outcomes, patients with VZV-related stroke face the same rehabilitation challenges as any ischaemic or haemorrhagic stroke patient, including physical therapy, speech therapy, and occupational therapy
The 2025 Frontiers in Neurology study of 108 unimmunocompromised patients underscores that even in people without obvious immune deficiency, outcomes can be serious, particularly when diagnosis is delayed.
PREVENTION, YOUR BEST DEFENCE IS VACCINATION
The most powerful tool available to prevent VZV brain complications is vaccination, both against chickenpox (to prevent primary infection) and against shingles (to prevent reactivation and its complications).
Chickenpox (Varicella) Vaccine
The chickenpox vaccine (a live attenuated VZV vaccine) is routinely given as a two-dose schedule in the United States:
• First dose: 12–15 months of age
• Second dose: 4–6 years of age
According to the CDC (2024), children who receive the chickenpox vaccine are significantly less likely to develop shingles, and therefore significantly less likely to develop neurological complications of reactivation, compared to those who had natural chickenpox infection.
Shingles Vaccine, Shingrix (RZV)
For adults who already carry latent VZV (virtually all adults over 50 in pre-vaccine generations), the recombinant zoster vaccine (RZV, Shingrix) is the most important preventive tool:
• Who should receive it: The CDC recommends two doses for all adults aged 50 and older, and for adults aged 19 and older with weakened immune systems (Updated April 24, 2024)
• Schedule: Two doses given 2–6 months apart (1–2 months apart for immunocompromised adults)
• Efficacy: Over 90% effective at preventing shingles in immunocompetent adults; also highly effective at reducing shingles severity, post-herpetic neuralgia, and neurological complications in those who do develop breakthrough shingles
• Not a live vaccine: Unlike the older Zostavax (which has been withdrawn), Shingrix uses a VZV protein antigen plus adjuvant, making it safe for immunocompromised individuals too
A 2025 study in allo-HSCT recipients found that vaccination with Shingrix significantly boosted anti-VZV antibody levels and reduced reactivation rates, supporting its use even in this very high-risk population.
PRACTICAL ACTION
If you are 50 or older and have not received Shingrix, speak to your doctor or pharmacist today. In the U.S., Shingrix is widely available at pharmacies without a specialist appointment. For immunocompromised adults from age 19, ask your specialist about the timing of vaccination.
→ Related: link to understanding vaccines
→ Related: link to Ebola and infectious disease
KEY TAKEAWAYS
✦ The varicella zoster virus, responsible for both chickenpox and shingles, can reactivate and invade the brain, causing two main syndromes: VZV encephalitis (brain tissue inflammation) and VZV vasculopathy (brain artery inflammation leading to stroke). VZV accounts for 5–8% of adult encephalitis cases.
✦ A hallmark danger: VZV brain inflammation can occur without a rash, and vasculopathy can develop weeks to months after a resolved shingles episode. This makes it chronically underdiagnosed. Any sudden neurological symptoms in a person with a history of recent shingles should raise suspicion.
✦ Diagnosis requires lumbar puncture with CSF PCR and VZV antibody testing, plus MRI and vascular imaging. PCR alone can be falsely negative; combined testing is recommended.
✦ IV acyclovir, started as early as possible, is the cornerstone of treatment, sometimes combined with corticosteroids (prednisolone or methylprednisolone) for the inflammatory component of vasculopathy. Speed of treatment initiation directly affects outcomes.
✦ Shingrix (recombinant zoster vaccine) is over 90% effective at preventing shingles and its neurological complications. The CDC recommends it for all adults aged 50+. Getting vaccinated is the single most actionable step available to reduce your risk.
CLOSING
VZV brain inflammation is one of those medical conditions that sits at a dangerous intersection: it’s uncommon enough that it doesn’t get the public attention it deserves, but serious enough that delayed recognition can be catastrophic. The virus that caused your childhood chickenpox has never left your body. For most people, it stays dormant forever. But understanding the signs that it has reactivated and reached the brain, and knowing that immediate emergency care is required could make the difference between full recovery and lasting neurological damage.
The bigger message, though, is prevention. The Shingrix vaccine is one of modern medicine’s most effective tools against a common latent virus with serious neurological potential. If you’re 50 or older and haven’t received it, please make that appointment. If you have immunocompromised family members aged 19 or older, ask their specialist about timing. And if you or someone you know develops sudden neurological symptoms, with or without a shingles rash, call emergency services immediately. Time saved is brain saved.