 |
| Photo from healthline.com |
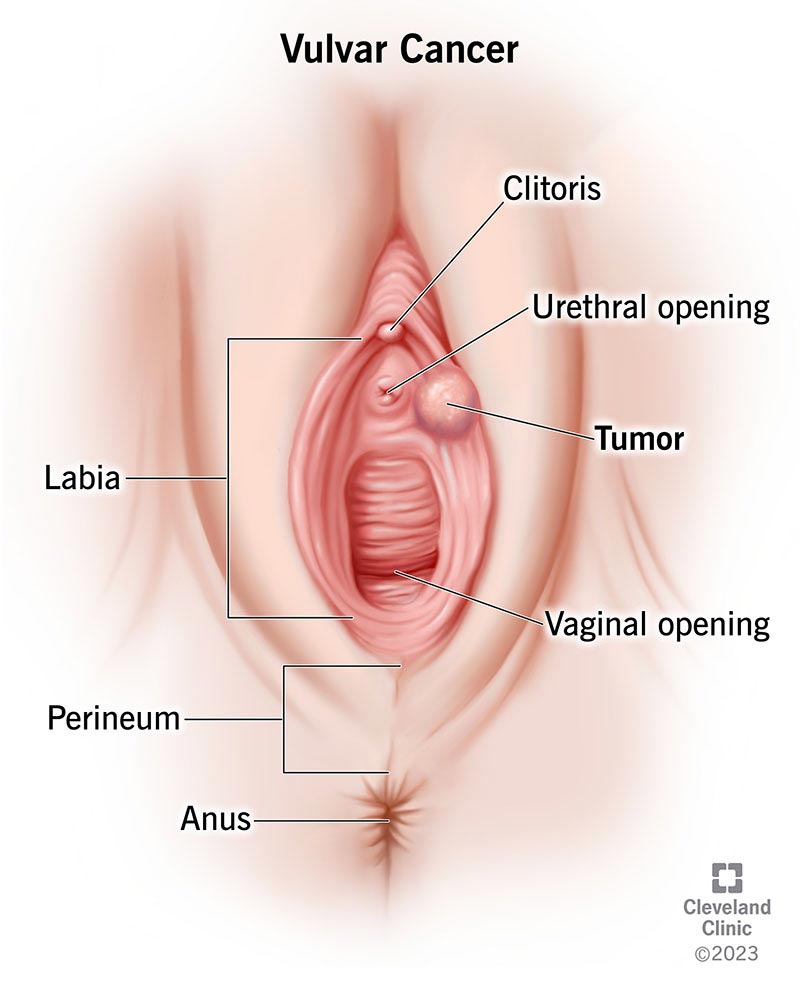
A woman’s vulva is her external genitalia. It is made up of the skin and fatty tissue that surrounds the clitoris and the vaginal and urethral openings. The fatty tissue forms two folds, the labia majora and labia minora, on either side of the vaginal opening. Cancer of the vulva is most commonly found in or on the labia. It can also occur on the clitoris or in Bartholin’s glands, which create a mucus-like lubricating fluid and are located on the sides of the vaginal entrance.
VULVAR CANCER
Cancer develops when healthy cells mutate and expand uncontrollably, generating a mass known as a tumor. A tumor might be malignant or noncancerous. A malignant tumor is one that can grow and spread to other regions of the body. A benign tumor is one that can develop but does not spread.
Vulvar cancer is named after the type of tissue in which it began. However, vulvar skin, like any other skin, can develop skin cancer. Squamous cell carcinoma is the most frequent kind of vulvar cancer. Other vulvar malignancies that are less prevalent include adenocarcinoma, melanoma, sarcoma, and verrucous carcinoma.
Squamous cell carcinoma: Squamous cell carcinoma is a form of skin cancer that accounts for over 90% of vulvar malignancies, the majority of which occur on the labia.
Squamous cancer can emerge from a “precancerous” state, which occurs when alterations in cells have the potential to become cancer but do not always do so. This is referred to as vulva intraepithelial neoplasia (VIN). VIN is a premalignant cell development on the vulva that is handled differently than invasive cancer. The term “premalignant” denotes that it is not yet cancer. VIN is further classified as “usual-type VIN” and “differentiated VIN” based on how the cells appear under a microscope. Usual-type VIN is more common in younger women and is linked to human papillomavirus (HPV). Differentiated VIN is less prevalent, more common in older women, and is not linked to HPV. Differentiated VIN is more common in women who have lichen sclerosus, a skin disorder that is commonly detected by a gynecologist and is a known condition prior to VIN, but not always. This type of VIN can progress to a fast-growing, aggressive squamous carcinoma.
Verrucous carcinoma: This is a wart-like, slow-growing form of squamous cell carcinoma.
Adenocarcinoma: Adenocarcinoma begins in the Bartholin’s glands, often known as vulvar sweat glands. It accounts for only a small proportion of vulvar cancers. It is most commonly observed on the sides of the vaginal entrance.
Melanoma: Melanoma is a kind of skin cancer that accounts for around 2% to 4% of all vulvar cancers. Melanoma is most commonly discovered on skin in areas of the body that are frequently exposed to the sun, but it can also grow in areas where there is no sun exposure. When it appears in the vulva, it usually appears on the clitoris or the labia minora. Women who have melanoma on other parts of their bodies are more likely to get vulvar melanoma. Vulvar melanoma is frequently treated with approaches similar to those used to treat melanoma in other regions of the body.
Sarcoma: Sarcoma is a connective tissue tumor that develops beneath the skin.
SYMPTOMS AND SIGNS OF VULVAR CANCER
Symptoms or indicators of vulvar cancer may include the following. A symptom, such as weariness, nausea, or discomfort, is something that only the person experiencing it can identify and explain. A sign is something that others can recognize and quantify, such as a fever, rash, or an increased pulse. Signs and symptoms, when combined, can assist describe a medical situation. People with vulvar cancer may not exhibit any of the signs and symptoms listed below. Alternatively, the origin of a symptom or sign could be a medical disease other than cancer.
- A lump or growth in or on the vulvar or groin area (an enlarged lymph node).
- A vulvar skin patch that is different in texture or color from the rest of the vulvar area.
- Itching, pain, soreness, or burning in the vulvar area that persists.
- Urination is excruciatingly painful.
- Bleeding or discharge that is not due to menstruation.
- An ulcer, open wound, or cut that has been present for more than one month.
- A modification to the appearance of an existing mole (this symptom is for vulvar melanoma specifically).
- Wart-like growths that look like genital warts.
Please consult your doctor if you are concerned about any changes you are experiencing. In addition to other questions, your doctor will inquire as to how long and how frequently you have been suffering any symptom. This is done to assist in determining the cause of the condition, which is referred to as a diagnostic.
If cancer is discovered, symptom relief is an important element of cancer care and treatment. This is known as palliative care or supportive care. It is frequently initiated shortly after diagnosis and continues throughout treatment. Make an appointment with your health care provider to discuss your symptoms, especially any new or changing symptoms.
STAGES OF VULVAR CANCER
Staging describes where the cancer is located, whether or not it has spread, and whether or not it is impacting other organs in the body. The stage of vulvar cancer is evaluated by performing surgery and assessing the removed tissues, including the vulva, the underlying and adjacent tissues, and the lymph nodes in the groin, which are small, bean-shaped organs that aid in infection fighting. Imaging scans are also employed in staging.
Knowing the stage allows the doctor to propose extra treatment if necessary and can assist estimate a patient’s prognosis, or the likelihood of recovery. Distinct forms of cancer have different stage descriptions. The staging system devised by FIGO, the International Federation of Obstetrics and Gynecology (Federation Internationale de Gynecologie et d’Obstetrique), is the most often used for vulvar cancer.
FIGO stages for vulvar cancer
 Doctors determine the cancer stage by examining the tumor and determining whether the cancer has spread to lymph nodes or other places of the body.
Doctors determine the cancer stage by examining the tumor and determining whether the cancer has spread to lymph nodes or other places of the body.The size of a tumor is measured in centimeters (cm). A centimeter is approximately the width of a normal pen or pencil. One centimeter (cm) is made up of ten millimeters (mm).
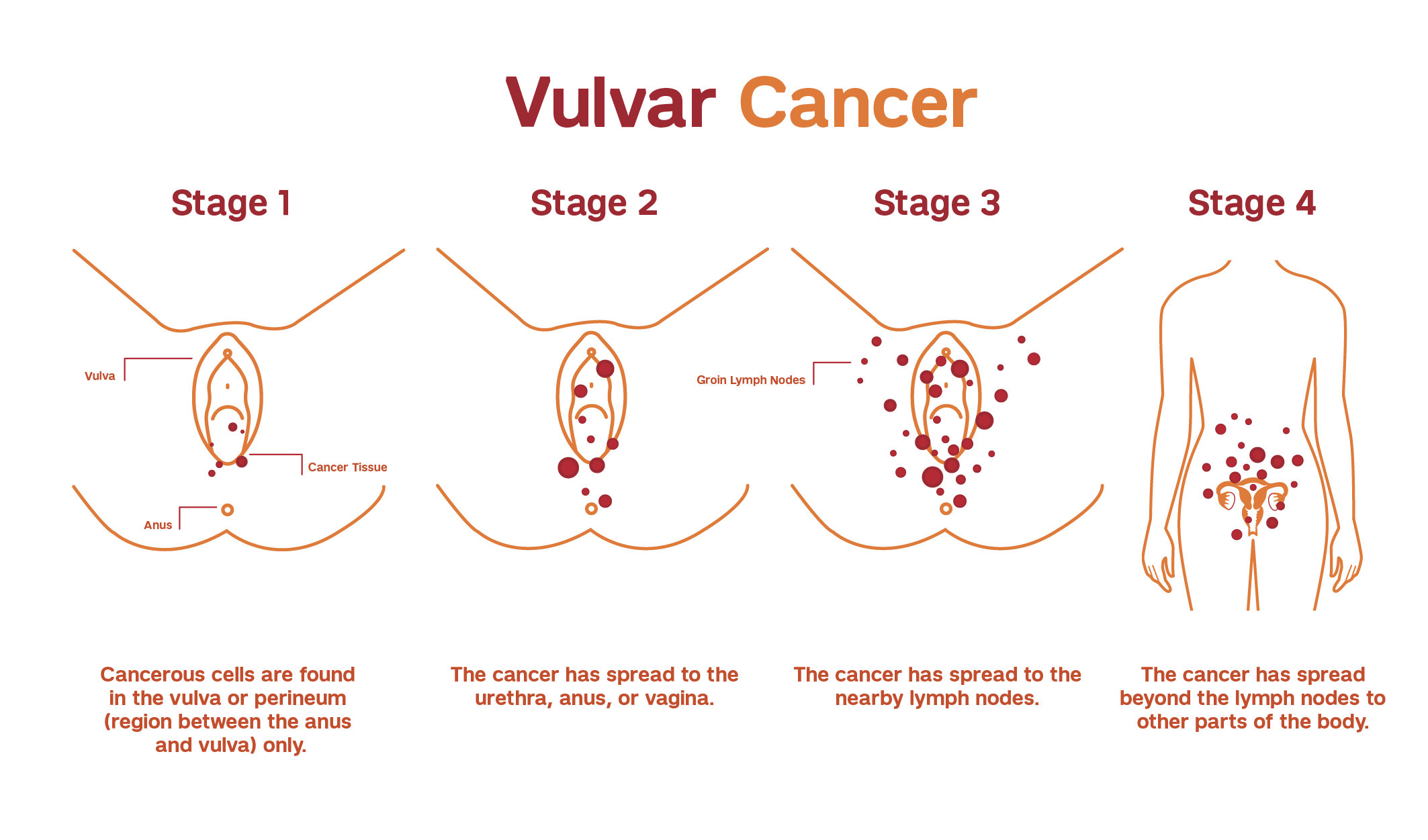
Stage I: Only the vulva or the vulva and perineum are affected by the tumor. It is not spreading.
- Stage IA: The tumor is limited to the vulva or the vulva and perineum, is 2 cm or less in size, has not spread, and is no deeper than 1 mm.
- Stage IB: The tumor is larger than cm in size or deeper than 1 mm, however it solely exists in the vulva or the vulva and perineum.
Stage II: The tumor has grown to any size and has spread to neighboring structures, such as the lower urethra, vagina, or anus. It has not spread to the lymph nodes or any other portion of the body.
Stage III: The cancer has spread to adjacent tissue, such as the vagina, anus, or urethra, as well as the lymph nodes in the groin. There are no far-flung metastases.
- Stage IIIA: The cancer has spread to surrounding tissue (the vagina, anus, or urethra). There are one or two metastases to lymph nodes, but they are less than 5 mm in size, or there is one metastasis that is 5 mm in size. There are no far-flung metastases.
- Stage IIIB: The cancer has spread to neighboring tissue (the vagina, anus, or urethra). There are 3 or more lymph node metastases, but they are less than 5 mm in size, or there are 2 or more 5 mm metastases. There are no far-flung metastases.
- Stage IIIC: The cancer has spread to neighboring tissue (the vagina, anus, or urethra) as well as one or more lymph nodes and the lymph node capsule, or covering, that surrounds them. There are no far-flung metastases.
Stage IV: The cancer has spread to the upper vaginal or urethral linings, or it has moved to a distant portion of the body.
- Stage IVA: The cancer has spread to the upper section of the urethra, vagina, or anus; it has spread to regional lymph nodes and caused ulceration; or it has adhered the lymph node to the tissue beneath it. There are no far-flung metastases.
- Stage IVB: The cancer has spread to another section of the body.
Recurrent cancer: Cancer that recurs after therapy is referred to as recurrent cancer. If the cancer returns, more tests will be performed to determine the degree of the recurrence. These tests and scans are frequently identical to those performed at the time of the first diagnosis. Vulvar tumors that return only on the vulva are frequently treatable.
DIAGNOSIS OF VULVAR CANCER
Many tests are used by doctors to detect or diagnose cancer. They also perform tests to see whether the cancer has spread to another place of the body from where it began. This is referred as as metastasis. Imaging tests, for example, can reveal whether or not the cancer has spread. Images of the inside of the body are produced via imaging tests. Doctors may also conduct tests to determine which treatments are most likely to be effective.
A biopsy is the only guaranteed way for a doctor to know if a part of the body has cancer in most cases of cancer. During a biopsy, the doctor extracts a small sample of tissue for laboratory testing. If a biopsy is not possible, the doctor may recommend alternative tests to aid in the diagnosis.
How is vulvar cancer diagnosed?
There are numerous tests available to diagnose vulvar cancer. Not all of the tests outlined here will be utilized on every individual. When selecting a diagnostic test, your doctor, gynecologist, or dermatologist may take the following things into account:
- The cancer type suspected
- Your symptoms and signs
- Your age and general well-being
- The outcomes of previous medical tests
The initial step in identifying vulvar cancer is a physical examination, which includes a pelvic exam. The doctor inspects the vulva before feeling the uterus, vagina, ovaries, bladder, and rectum for any unexpected changes.
The following tests, in addition to a physical examination, may be used to identify vulvar cancer:
- Biopsy: A biopsy is the removal of a small sample of tissue for microscopic examination. Other tests can indicate the presence of cancer, but only a biopsy can provide a definitive diagnosis. A pathologist examines the sample taken during the biopsy. A pathologist is a medical professional who specializes in interpreting laboratory tests and assessing cells, tissues, and organs to identify disease. The sort of biopsy used will be determined by the location of the questionable tissue.
If the biopsy reveals invasive vulvar cancer, the woman will be referred to a gynecologic oncologist, a doctor who specializes in treating this form of cancer.
- Chest x-ray: An x-ray is a technique that uses a small amount of radiation to create a picture of the structures inside the body. A chest x-ray may be performed to determine whether the cancer has progressed to the lungs.
- Colposcopy: A colposcopy may be performed by the doctor to evaluate the vagina, vulva, and cervix for any abnormalities, especially if Pap or HPV tests show abnormal results. A colposcope is a specific tool that magnifies the surface of the cervix, vagina, and vulva. It is comparable to a microscope. The colposcope illuminates and magnifies these areas for the doctor. The colposcope is not placed within the woman’s body. The examination is unpleasant but not painful, may be performed in the doctor’s office, and has no side effects. This examination is safe for pregnant women.
- Magnetic resonance imaging (MRI): An MRI produces detailed images of the body by using magnetic fields rather than x-rays. The tumor’s size can be determined via an MRI. To provide a crisper image, a special dye known as a contrast medium is administered before to the scan. Typically, this dye is injected into a patient’s vein.
- Endoscopy: An endoscopy allows the doctor to view within the body using an endoscope, which is a narrow, illuminated, flexible tube. The patient may be sedated while the tube is introduced through the urethra into the bladder, a procedure known as cystoscopy, or through the anus into the rectum, a procedure known as proctoscopy or colonoscopy. Sedation is the administration of drugs in order to become more relaxed, tranquil, or sleepy.
- Computed tomography (CT) scan: A CT scan uses x-rays captured from various angles to create images of the inside of the body. A computer combines these images to create a detailed, three-dimensional image that identifies any anomalies or tumors. A CT scan can be performed to determine the size of the tumor. To improve image detail, a specific dye known as a contrast medium is sometimes administered before to the scan. This dye can be injected into a patient’s vein or administered orally and ingested, typically as a liquid.
- Positron emission tomography (PET) or PET-CT scan: A PET scan is frequently coupled with a CT scan to form a PET-CT scan. However, your doctor may refer to this technique simply as a PET scan. A PET scan is a technique for creating images of organs and tissues within the body. A radioactive sugar compound is put into the patient’s body in modest amounts. This sugar molecule is absorbed by the cells that consume the most energy. Cancer absorbs more radioactive stuff because it aggressively uses energy. The amount of radiation in the material, however, is too low to be dangerous. The material is then detected by a scanner, which produces images of the inside of the body.
TREATMENT OF VULVAR CANCER
Different types of specialists frequently collaborate in cancer care to develop a patient’s overall treatment plan, which mixes many sorts of therapy. This is referred to as a multidisciplinary team. Vulvar cancer surgery is performed by gynecologic oncologists, and radiation oncologists and medical oncologists may also be engaged in the treatment of vulvar cancer. Pathologists and radiologists assist in confirming the diagnosis and determining the extent of disease. Other health care professionals on cancer care teams include physician assistants, nurse practitioners, oncology nurses, social workers, pharmacists, counselors, nutritionists, and others.
The most prevalent types of vulvar cancer treatment are outlined below. Your treatment plan will also include treatment for symptoms and side effects, which is an important aspect of cancer care.
Treatment options and recommendations for vulvar cancer are influenced by a variety of factors, including the type and stage of the disease, potential side effects, and the patient’s preferences and overall health. Take the time to read about all of your treatment options, and don’t be afraid to ask clarifying questions. Discuss the aims of each treatment with your doctor, as well as what you can expect during treatment. These discussions are known as “shared decision-making.” When you and your doctors collaborate to identify therapies that meet the goals of your care, this is referred to as shared decision-making. Because there are various treatment choices for vulvar cancer, shared decision-making is very vital.
Concerns about sexual health and the possibility of having children
People suffering from vulvar cancer may be concerned about how their treatment will effect their sexual health and fertility. Before beginning treatment, these topics should be reviewed with the health care team. Premenopausal women who are still fertile and want to protect their fertility may be sent to a reproductive endocrinologist (REI) before beginning therapy. It may be beneficial to discuss whether fertility preservation options are covered by health insurance.
Vulvar cancer treatments
 Surgery is the primary treatment for vulvar cancer. If a biopsy reveals that vulvar cancer is present and looks to be limited to the vulva, most people will have surgery. If the cancer cannot be completely removed with surgery, if the cancer has a high chance of recurrence, and/or if the disease is discovered in lymph nodes, radiation therapy and chemotherapy may be employed.
Surgery is the primary treatment for vulvar cancer. If a biopsy reveals that vulvar cancer is present and looks to be limited to the vulva, most people will have surgery. If the cancer cannot be completely removed with surgery, if the cancer has a high chance of recurrence, and/or if the disease is discovered in lymph nodes, radiation therapy and chemotherapy may be employed.If the tumor has advanced to the point that surgical excision is no longer an option, the treatment approach may include radiation therapy, followed by low-dose chemotherapy administered weekly (typically with cisplatin, which is a generic medicine) at the same time as the radiation treatments. This method is known as “chemoradiation.” If the entire tumor does not disappear after these therapies, surgical excision of the vulvar lesion is occasionally contemplated.
Surgery
During a surgery, the tumor and some surrounding healthy tissue are removed. A gynecologic oncologist is a specialist who specializes in the surgical treatment of gynecologic cancer. The sort of surgery performed is carefully examined due to the position and sensitivity of vulvar tissue. The following surgical options are available for invasive vulvar cancer:
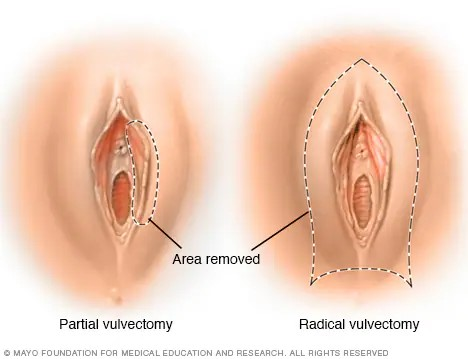
Vulvectomy: Depending on the size and spread of the initial tumor, a vulvectomy may involve the removal of part or all of the vulva. Among the several vulvectomy techniques used to treat invasive vulvar cancer are:
- Radical local excision of the vulva: This procedure is performed to remove the tumor as well as a substantial quantity of tissue surrounding it, known as a margin. It is often employed when the tumor is smaller than 4 centimeters (cm) in diameter and is either stage I or stage II illness.
- Modified radical vulvectomy: This word refers to a surgical operation in which only a portion of the vulva is removed. In a radical hemivulvectomy, for example, only one side of the vulva is removed.
- Radical vulvectomy: A radical vulvectomy is the surgical removal of a portion or all of the vulva, as well as the underlying deep tissue. Because most vulvectomies are modified in some way, and very large tumors are usually treated with chemoradiation, as explained below, this is a very uncommon operation.
Laser surgery: A concentrated beam of light is utilized in this therapy to melt a precancerous skin lesion. It cannot be utilized to treat a cancerous tumor that has spread throughout the body.
Lymphadenectomy: During surgery, groin lymph nodes, also known as inguinal-femoral lymph nodes, are frequently removed to determine whether the cancer has progressed to the lymph nodes. Lymphadenectomy is the surgical operation used to remove lymph nodes. If the cancer is just on one side of the vulva, the lymph nodes in the groin on that side may only need to be removed. Only the nearest lymph node, known as a sentinel lymph node, may need to be removed for a minor vulvar tumor.
Before undergoing surgery, consult with your health care team about the potential adverse effects of the procedure.
Coping with vulvar surgery
It is common to feel a variety of feelings following vulvar surgery, such as loss, sadness, or anxiety. Some women may feel as if they have lost a piece of their femininity. Others are concerned about whether sexual activity can resume following surgery. People may also be concerned about the impact of the operation on their relationships with their spouses.
Before surgery, it is critical to discuss the operation with the surgeon, as well as the potential adverse effects and when sexual intercourse can resume. People should talk to their doctors about where they can get further information or help coping with this type of surgery.
Chemoradiation therapy for advanced-stage vulvar cancers
To decrease a large vulvar tumor before surgery, radiation therapy is frequently paired with low-dose chemotherapy. This is referred to as chemoradiation therapy. This treatment can help to avoid the need for vulva removal and lessen the amount of tissue removed. Chemotherapy is administered together with radiation therapy. This therapeutic approach is critical when the tumor involves the urethra or anus, as it allows urine and bowel function to be preserved.
Radiation therapy
The use of high-energy x-rays or other particles to eliminate cancer cells is known as radiation therapy. A radiation oncologist is a doctor who specializes in the use of radiation therapy to treat cancer. Radiation therapy can be performed either before or after surgery to diminish the size of the tumor or to eradicate any leftover cancer cells.
External-beam radiation therapy, which delivers radiation from a machine outside the body, is the most prevalent method of radiation treatment. Internal radiation therapy, also known as brachytherapy, is a type of radiation therapy that uses implants to deliver radiation. A radiation therapy regimen, or schedule, typically consists of a predetermined number of treatments administered over a predetermined time period.
Radiation therapy can cause fatigue, mild to severe skin reactions, upset stomach and loose bowel motions, damage to healthy vaginal tissue, and vaginal constriction. The majority of these side effects fade quickly when treatment is completed. However, the vagina may shorten and narrow to the point that sexual intercourse is no longer viable. To avoid this, the vagina may need to be stretched many times per week with a plastic tube known as a vaginal dilator. To avoid permanent constriction or shortening, it is preferable to begin using a vaginal dilator during or shortly after your therapy.
The effects of radiation therapy on vaginal and vulvar tissue may appear or vary for months to years after treatment is completed. Before beginning therapy, discuss with your doctor any potential side effects and how to manage them.
Chemotherapy
 Medication-based treatments are used to kill cancer cells. Medication may be administered via the bloodstream in order to reach cancer cells throughout the body. When a medicine is administered in this manner, it is referred to as systemic therapy. Medication can also be administered locally, which means that it is applied directly to the cancer or is retained in a certain portion of the body.
Medication-based treatments are used to kill cancer cells. Medication may be administered via the bloodstream in order to reach cancer cells throughout the body. When a medicine is administered in this manner, it is referred to as systemic therapy. Medication can also be administered locally, which means that it is applied directly to the cancer or is retained in a certain portion of the body.A gynecologic oncologist or a medical oncologist, a clinician who specializes in treating cancer with drugs, will prescribe systemic therapy for vulvar cancer. Medications are frequently administered by an intravenous (IV) tube inserted into a vein with a needle, or in the form of a pill or capsule that is eaten (orally). If you are given oral drugs, make sure to ask your health care team how to store and manage them securely.
Chemotherapy is a sort of systemic therapy used to treat vulvar cancer. Chemotherapy is the use of medications to eradicate cancer cells, typically by preventing the cancer cells from growing, dividing, and proliferating.
A chemotherapy regimen, or schedule, typically consists of a predetermined number of treatments administered over a predetermined time period. A patient may be administered one medicine at a time or a mixture of drugs at the same time.
If the patient is going to have external radiation therapy for locally advanced vulvar cancer, cisplatin chemotherapy is occasionally given intravenously every week at the same time as the radiation therapy.
If the cancer has expanded beyond the pelvis or recurred, doctors may explore employing medications used to treat cervical cancer and vaginal cancer, both of which are squamous cell gynecologic cancers caused by HPV.
Patients with metastatic vulvar cancer are often treated with platinum-based combination chemotherapy, typically carboplatin (a generic medication) and paclitaxel (Taxol). Bevacizumab (Avastin, Mvasi) is a targeted treatment that is sometimes added to this combination.
Chemotherapy side effects vary depending on the individual, as well as the medications and doses employed. Fatigue, infection risk, nausea and vomiting, hair loss, lack of appetite, or diarrhea are some of the symptoms. These adverse effects normally fade away once the treatment is completed.
The patient’s overall health, kidney function as assessed by laboratory testing, and other medical considerations all influence whether or not these medicines are taken.
Cancer treatments are always being researched and tested. Talking with your doctor is often the best method to understand about the medications your doctor has prescribed for you, their purpose, and any potential adverse effects or interactions with other medications.
It is also critical to inform your doctor if you are using any other prescription, over-the-counter, or herbal drugs or supplements. Herbs, vitamins, and other pharmaceuticals can interact with cancer therapies, resulting in unpleasant side effects or decreased efficacy.
Metastatic vulvar cancer
Doctors refer to cancer that has spread to another place of the body from where it began as metastatic cancer. Chemotherapy or immunotherapy may be advised in this scenario. Immunotherapy is a sort of systemic cancer treatment that increases the body’s inherent anti-cancer defenses. It employs compounds produced by the body or in a laboratory to increase the ability of your immune system to detect and eliminate cancer cells. As previously stated, the medications used to treat the majority of metastatic vulvar cancer are often the same as those used to treat metastatic cervical cancer.
It is advisable to consult with experts who have treated metastatic vulvar cancer, such as gynecologic or medical oncologists. Different doctors may have differing views on the optimal conventional treatment strategy. Clinical trials are another possibility. Learn more about getting a second opinion before beginning treatment so that you are confident in your treatment plan.
Your treatment strategy may contain a combination of the above-mentioned treatments. Palliative treatment will also be essential in order to alleviate symptoms and negative effects.
A diagnosis of metastatic cancer is extremely stressful and challenging for the majority of people. You and your family are encouraged to express your feelings to doctors, nurses, social workers, and other members of the health care team. Talking with other patients, such as in a support group or other peer support program, may also be beneficial.
Remission and the possibility of recurrence
When cancer cannot be identified in the body and there are no symptoms, the patient is said to be in remission. This is often known as having “no evidence of illness,” or NED.
Remission can be either temporary or permanent. Many people are concerned that the cancer will recur as a result of this uncertainty. While many remissions are lasting, it is critical to discuss with your doctor the likelihood of the cancer returning and what steps would be taken to monitor for a recurrence. Understanding your recurrence risk and treatment options may make you feel more prepared if the cancer returns.
Recurrent cancer occurs when the cancer returns after the initial treatment. It may return in the same location (called a local recurrence), nearby (called a regional recurrence), or elsewhere (distant recurrence).
When this happens, a new round of testing will begin in order to understand as much as possible about the recurrence. Following the completion of this testing, you and your doctor will discuss treatment choices. The treatments outlined above, such as surgery, chemotherapy, and radiation therapy, are frequently included in the treatment plan, but they may be used in a different mix or delivered at a different pace than those used during initial treatment. Your doctor may recommend that you participate in clinical studies that are looking for new ways to treat this sort of recurring cancer. Your doctor may also wish to perform biomarker testing on your tumor to assist guide future treatment decisions, which is known as molecular or targeted tumor testing. Palliative care will be essential for reducing symptoms and side effects regardless of the treatment plan you choose.
People suffering from recurring cancer may experience emotions such as bewilderment or anxiety. You are urged to discuss these feelings with your health care provider and inquire about support options to assist you in coping.

