- Pain and cramps in the abdomen
Please consult your doctor if you are concerned about any changes you are experiencing. In addition to other questions, your doctor will inquire as to how long and how frequently you have been experiencing the symptom(s). This is done to determine the source of the problem, which is referred to as a diagnostic.
If cancer is discovered, symptom relief is an important element of cancer care and treatment. This is known as “palliative care” or “supporting care.” It is frequently initiated shortly after diagnosis and continues throughout treatment. Make an appointment with your health care provider to discuss your symptoms, especially any new or changing symptoms.
WHAT ARE THE STAGES OF GALLBLADDER CANCER?
Staging describes where the cancer is present, whether or not it has spread, and whether or not it is impacting other sections of the body. Doctors use diagnostic tests to determine the stage of cancer, so staging may not be complete until all tests are completed. Knowing the stage allows the doctor to propose the best treatment and anticipate a patient’s prognosis, which is the likelihood of recovery or average life expectancy. Distinct forms of cancer have different stage descriptions.
TNM system of staging
The TNM system is one technique that clinicians use to describe the stage. Doctors use diagnostic test and scan results to address the following questions:
- Tumor(T): What is the size of the main tumor? Where can I find it?
- Node(N): Has the cancer spread to your lymph nodes? If so, where are they and how many are there?
- Metastasis(M): Is the cancer spreading to other places of the body? If so, where and how much?

The results are combined to establish each person’s stage of gallbladder cancer. There are five stages: stage 0 (zero), stages I through IV (1 through 4). The stage provides a common language for doctors to describe the cancer so that they can collaborate to determine the best treatments.
Staging can be classified as “clinical” or “pathological.” Clinical staging is determined by the results of pre-surgery diagnostics, which may include physical examinations and imaging tests. Pathological staging is determined by what is discovered during surgery, including a biopsy. Pathological staging, in general, gives the most comprehensive information for determining a patient’s prognosis.
More information on each component of the TNM system for gallbladder cancer may be found below:
Tumor (T)
The “T” plus a letter or number (0 to 4) is used in the TNM system to denote the quantity of malignancy identified in the gallbladder. The size of a tumor is measured in millimeters (cm). A centimeter is approximately the width of a normal pen or pencil.
Stages can also be subdivided into smaller groups to assist describe the tumor in greater detail. This enables the doctor to devise the most effective treatment strategy for each patient. The information for each tumor stage is shown below.
TX: There is no way to evaluate the original tumor.
T0: There was no sign of cancer in the gallbladder.
Tis: This term refers to carcinoma (cancer) in situ, which suggests that the tumor is still in a pre-invasive form and that any spread, if any, is quite limited.
T1: The tumor has only penetrated the lamina propria (a type of connective tissue found beneath the thin layer of tissue covering a mucous membrane) or muscle layer of the gallbladder.
- T1a: Invasion of the tumor into the lamina propria.
- T1b: The tumor has spread into the muscle layer.
T2: The tumor has penetrated the perimuscular connective tissue (the layer between the muscle layer and the serosa) but has not spread to the liver or beyond the serosa (the outer layer).
- T2a: On the peritoneal side, the tumor has penetrated the perimuscular connective tissue.
- T2b: The tumor has penetrated the perimuscular connective tissue on the liver’s side but has not spread.
T3: The tumor has spread beyond the gallbladder and/or has invaded the liver and/or at least one other neighboring organ or structure, such as the stomach, duodenum (a section of the small bowel), colon, or pancreas.
T4: The tumor has infiltrated the major portal vein or hepatic artery, or it has invaded more than one organ or structure other than the liver.
Node (N)
The letter “N” in the TNM staging system denotes lymph nodes. These little, bean-shaped organs aid in the fight against infection. Regional lymph nodes are lymph nodes located near the gallbladder. Lymph nodes located in other sections of the body are referred to as distant lymph nodes.
NX: The lymph nodes in the region cannot be evaluated.
N0: There is no metastases or spread of regional lymph nodes.
N1: There is lymph node metastases in the region.
N2: There is metastases to distant lymph nodes.
Metastasis (M)
The “M” in the TNM system indicates if the cancer has migrated to other parts of the body, a condition known as metastasis.
M0: There is no evidence of distant metastases.
M1: The cancer has spread to one or more other regions of the body.
Cancer stage grouping
Doctors determine the cancer stage by integrating the T, N, and M classifications.
Stage 0: Describes cancer in its early stages (Tis, N0, M0).
Stage I: A tumor that has just affected the gallbladder and has not spread (T1, N0, M0).
Stage II: The tumor has progressed to the perimuscular connective tissue but not elsewhere (T2, N0, M0).
Stage IIIA: A tumor has migrated beyond the gallbladder but has not reached adjacent arteries or veins. It has not spread to any of the body’s lymph nodes or other organs (T3, N0, M0).
Stage IIIB: A tumor of any size has spread to neighboring lymph nodes but not to nearby arteries and/or veins or to other areas of the body (T1, T2, T3; N1; M0).
Stage IVA: A tumor has spread to surrounding arteries, veins, and/or lymph nodes but not to distant areas of the body (T4, N0 or N1, M0).
Stage IVB: Any tumor that has spread to other parts of the body (any T, any N, M1) or any tumor that has distant lymph node dissemination, even if it has not gone to distant organs, is classified as Stage IVB (any T, N2, M0).
Recurrent: The term “recurrent gallbladder cancer” refers to cancer that has returned after treatment. If the cancer recurs, it may need to be staged again (a process known as re-staging) following the system described above. If the cancer returns, more tests will be performed to determine the degree of the recurrence. These tests and scans are frequently identical to those performed at the time of the first diagnosis. The most common recurrent disease is stage IV.
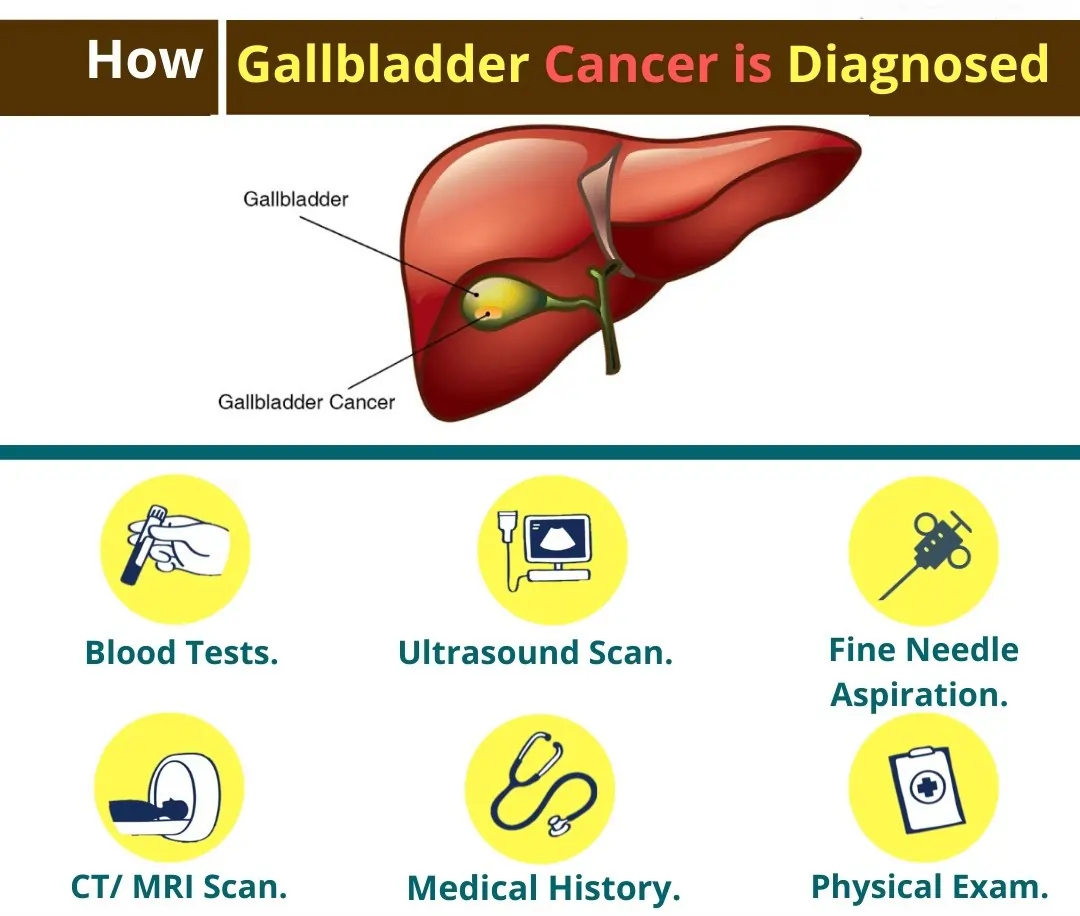
HOW IS GALLBLADDER CANCER DIAGNOSED?
Many tests are used by doctors to detect or diagnose cancer. They also perform tests to see whether the cancer has spread to another place of the body from where it began. This is referred as as metastasis. Imaging tests, for example, can reveal whether or not the cancer has spread. Images of the inside of the body are produced via imaging tests. Doctors may also conduct tests to determine which treatments are most likely to be effective.
A biopsy is the only guaranteed way for a doctor to know if a part of the body has cancer in most cases of cancer. During a biopsy, the doctor extracts a small sample of tissue for laboratory testing. If a biopsy is not possible, the doctor may recommend alternative tests to aid in the diagnosis.
There are numerous tests available to diagnose gallbladder cancer. Not all of the tests outlined here will be utilized on every individual. When selecting a diagnostic test, your doctor may take the following variables into account:
- The cancer type suspected
- Your age and general well-being
- The outcomes of previous medical tests
The following tests, in addition to a physical examination, may be used to diagnose gallbladder cancer:
Biopsy: A biopsy is the removal of a small sample of tissue for microscopic examination. Other tests can indicate the presence of cancer, but only a biopsy can provide a definitive diagnosis. The material is next examined by a pathologist. A pathologist is a medical professional who specializes in interpreting laboratory tests and assessing cells, tissues, and organs to identify disease.
Tissue samples can be obtained in one of numerous ways:
- With laparoscopy, a minimally invasive surgical method
- With a tiny needle or thick needle aspiration (a core biopsy), a computed tomography (CT or CAT) scan or ultrasound is used to guide needle insertion.
- In some situations, a biopsy is performed by inserting an endoscope (a thin, flexible tube with a strong light) into the mouth, through the stomach, and into the first part of the intestine. A instrument can be passed from the endoscope through the intestinal wall to extract a sample of tissue.
Endoscopic retrograde cholangiopancreatography (ERCP): An ERCP lets the doctor to look into the patient’s body. The patient is sedated briefly before the doctor inserts an endoscope via the mouth, down the esophagus, and into the stomach and small bowel. A smaller tube or catheter is inserted into the bile ducts via the endoscope. A dye is injected into the ducts, and x-rays are taken to determine whether a tumor is present in the area around the bile ducts. During an ERCP, a plastic or metal stent can be inserted across a clogged bile duct to assist reduce jaundice if it is present. This procedure should be carried out by an experienced gastroenterologist. A gastroenterologist is a doctor who specializes in gastrointestinal function and problems. This operation is more usually used to detect bile duct cancer than gallbladder cancer, however it may be done if gallbladder cancer spreads and plugs the bile ducts.
Percutaneous cholangiography: A tiny needle is introduced through the skin and into the gallbladder area during this surgery. A dye is injected through the needle to produce a clear image on x-rays. The doctor may be able to see if there is a tumor in the gallbladder by looking at the x-rays. A cholangiography, which is more often used, offers images of the bile ducts but may not reveal a tumor in the gallbladder. The method, on the other hand, is quite good in detecting the location of a blocked bile duct.
Laparoscopy: An endoscope is used during laparoscopy to examine the gallbladder and other interior organs. The tube is introduced into the abdomen through a tiny incision.
Computed tomography (CT or CAT) scan: A CT scan uses x-rays from various angles to create images of the inside of the body. A computer combines these images to create a detailed, three-dimensional image that shows any anomalies or malignancies. A CT scan can be used to determine the size of a tumor. To improve image detail, a specific dye called a contrast medium is sometimes administered prior to the scan. This dye can be injected into a patient’s vein or given to them as a tablet or liquid to ingest.
Magnetic resonance imaging (MRI): An MRI produces detailed images of the body by using magnetic fields rather than x-rays. It can be utilized to determine whether or not the malignancy has gone beyond the gallbladder. MRI can also be used to determine the size of a tumor. To provide a crisper image, a special dye known as a contrast medium is administered before to the scan. This dye can be injected into a patient’s vein or given to them in the form of a pill or liquid to consume.
MRI cholangiopancreatography refers to a type of MRI that is used to examine the gallbladder (MRCP). To obtain a crisper image, a contrast material may be administered before to the MRI.
Blood tests: The doctor may draw blood samples from the patient to check for high levels of bilirubin and other chemicals. Bilirubin is a substance that can accumulate in high quantities at people with gallbladder cancer due to tumor obstruction of the common bile duct. CA19-9 (carbohydrate antigen 19-9), a tumor marker, may also be tested in this form of malignancy. A tumor marker is a chemical produced by a tumor that can be detected in the blood and may be found at higher levels if cancer is present.
Ultrasound: An ultrasound creates a picture of the interior organs by using sound waves. Tumors produce distinct sound wave echoes than normal tissue. This implies that when the waves are bounced back to a computer and generate images, the doctor will be able to pinpoint a mass inside the body.
Endoscopic ultrasonography: Following sedation, a particular endoscope, which is a long, flexible scope, is inserted into the mouth. It has the ability to enter the stomach and some of the intestine. It features an ultrasonic probe at the end that can be used to look for tumors and guide a small needle biopsy.
Positron emission tomography (PET) or PET-CT scan: A PET scan is frequently coupled with a CT scan to form a PET-CT scan. However, your doctor may refer to this technique simply as a PET scan. A PET scan is a technique for creating images of organs and tissues within the body. A radioactive sugar compound is put into the patient’s body in modest amounts. This sugar molecule is absorbed by the cells that consume the most energy. Cancer absorbs more radioactive stuff because it aggressively uses energy. The amount of radiation in the material, however, is too low to be dangerous. The material is then detected by a scanner, which produces images of the inside of the body. These tests can be challenging to interpret at times because healthy and active tissues both actively use energy.
WHAT ARE THE TREATMENTS OF GALLBLADDER CANCER?
Different types of specialists frequently collaborate in cancer care to develop a patient’s overall treatment plan, which mixes many sorts of therapy. This is referred to as a multidisciplinary team. A gastroenterologist, a surgeon, a medical oncologist, and a radiation oncologist may be part of the team of clinicians treating gallbladder cancer. Other health care professionals on cancer care teams include physician assistants, nurse practitioners, oncology nurses, social workers, pharmacists, counselors, nutritionists, and others.
The most frequent types of gallbladder cancer therapies are mentioned below. Your treatment plan will also include treatment for symptoms and side effects, which is an important aspect of cancer care. Gallbladder cancer can be treated with one or more of the following methods: surgery, chemotherapy, or radiation therapy. Gallbladder cancer has a far better chance of being effectively treated if detected early.
The type and stage of cancer, potential side effects, and the patient’s preferences and overall health all influence treatment options and recommendations. Take the time to educate yourself on all of your therapy options. Make sure to clarify any points that are unclear. Discuss the aims of each treatment with your doctor, as well as what you can expect during treatment. These discussions are known as “shared decision-making.” When you and your doctors collaborate to identify therapies that meet the goals of your care, this is referred to as shared decision-making. Because there are various treatment options for gallbladder cancer, shared decision-making is especially important.
Surgery
During a surgery, the tumor and some surrounding healthy tissue are removed. A general surgeon, surgical oncologist, or hepatobiliary surgeon can do this procedure. A surgical oncologist is a specialist who specializes in the surgical treatment of cancer. A hepatobiliary surgeon specializes in liver, gallbladder, and bile duct surgery.
Gallbladder cancer is treated with the following forms of surgery:
Cholecystectomy: This treatment, also known as a simple cholecystectomy, includes the removal of the gallbladder. The gallbladder, 1 inch or more of liver tissue lying close to the gallbladder, and all lymph nodes in the region are all removed during an extended cholecystectomy.
Radical gallbladder resection: The gallbladder, a wedge-shaped piece of the liver around the gallbladder, the common bile duct, part or all of the ligaments between the liver and the intestines, and the lymph nodes around the pancreas and associated blood arteries are all removed during this treatment. Even if a basic cholecystectomy has already been performed, this operation may be advised for a more comprehensive resection to eliminate potentially malignant cells.
Palliative surgery: Even if the tumor cannot be completely removed, surgery can occasionally help ease symptoms caused by gallbladder cancer. For example, surgery may be used to clear a blockage in the bile ducts or intestines, or to stop bleeding.
The adverse effects will vary depending on the type of operation. Before undergoing surgery, consult with your health care team about the potential adverse effects of the procedure.
Radiation therapy
The use of high-energy x-rays or other particles to eliminate cancer cells is known as radiation therapy. A radiation oncologist is a doctor who specializes in the use of radiation therapy to treat cancer. External-beam radiation therapy, which is radiation delivered from a machine outside the body, is the most commonly used method of radiation treatment for gallbladder cancer. A radiation therapy regimen, or schedule, typically consists of a predetermined number of treatments administered over a predetermined time period.
Radiation therapy can be performed either before or after surgery to diminish the size of the tumor or to eradicate any leftover cancer cells. In some circumstances, radiation treatment is administered during surgery to directly target the tumor while protecting vital organs from the effects of standard radiation therapy. This is known as intra-operative radiation treatment, or IORT.
Chemoradiotherapy is a treatment that combines radiation therapy and chemotherapy. Chemoradiotherapy may be used after surgery and chemotherapy to eliminate any leftover cancer cells if a “positive margin” can be observed under a microscope. A positive margin indicates the presence of cancer cells on the edge of the tissue removed during surgery, which may indicate that there are still very minute amounts of cancer cells in the patient’s body that can potentially grow further.
Because radiation therapy is not always used to treat gallbladder cancer, your doctor may or may not advise it. Fatigue, moderate skin reactions, upset stomach, loose bowel motions, and damage to adjacent structures such as the liver or intestines are all possible side effects of radiation therapy. The majority of negative effects fade quickly after treatment is completed.
Chemotherapy
Chemotherapy is the use of medications to eradicate cancer cells, typically by preventing the cancer cells from growing, dividing, and proliferating.
A chemotherapy regimen, or schedule, typically consists of a predetermined number of cycles administered over a predetermined time period. A patient may be administered one medicine at a time or a mixture of drugs at the same time.
Chemotherapy should be administered following surgery to assist prevent a recurrence. Capecitabine (Xeloda) is recommended by ASCO for 6 months after surgery. After surgery, people with hilar cholangiocarcinoma and extrahepatic cholangiocarcinoma may get chemoradiotherapy and capecitabine to eliminate leftover cancer cells if a positive margin can be observed under a microscope. A positive margin indicates the presence of cancer cells in the area where the tumor was excised.
Gemcitabine (Gemzar), fluorouracil (5-FU), cisplatin (Platinol), oxaliplatin (Eloxatin), and nab-paclitaxel are some of the other medications widely used to treat gallbladder cancer (Abraxane). Chemotherapy side effects vary according to the individual and the dose administered, but they can include exhaustion, infection risk, nausea and vomiting,
hair loss, loss of appetite, diarrhea, neuropathy, and edema. These adverse effects normally fade away once the treatment is completed.
Chemotherapy is typically used as palliative care for gallbladder cancer. It may be advised after the tumor has been surgically removed. Neoadjuvant chemotherapy refers to chemotherapy administered prior to surgery. Adjuvant chemotherapy refers to chemotherapy administered as an extra therapy following surgery.
Immunotherapy
Immunotherapy, also known as biologic therapy, is intended to increase the body’s natural defenses against cancer. It employs components created by the body or in a laboratory to enhance, target, or restore
immune system activity.
Pembrolizumab (Keytruda) and nivolumab (Opdivo) are two immunotherapy medications that have been approved for all MSI-H malignancies, including MSI-H gallbladder tumors. MSI is a genomic marker that signals a problem with a cell’s ability to repair damaged DNA, which can result in an increase in genetic alterations, or mutations. These mutations cause aberrant proteins to be produced on tumor cells, allowing immune cells to more quickly locate and kill the tumor.
Different forms of immunotherapy might result in a variety of adverse effects. Skin rashes, flu-like symptoms, diarrhea, and weight fluctuations are all common adverse effects. Consult your doctor about the potential adverse effects of the immunotherapy that has been prescribed for you.
Metastatic gallbladder cancer
Doctors refer to cancer that has spread to another place of the body from where it began as metastatic cancer. If this occurs, it is a good idea to consult with experts who have treated similar cases, especially since this is a rare malignancy. Different doctors may have differing views on the optimal conventional treatment strategy. Clinical trials are another possibility.
Surgery, medicines, or radiation therapy may all be part of your treatment plan. Palliative treatment will also be essential in order to alleviate symptoms and negative effects.
A diagnosis of metastatic cancer can be extremely stressful and traumatic for many people. Doctors, advanced practice providers, nurses, social workers, and other members of the health care team encourage you and your family to express your feelings to them. Talking with other patients, such as in a support group or other peer support program, may also be beneficial.