|
| Photo from emedicinehealth.com |
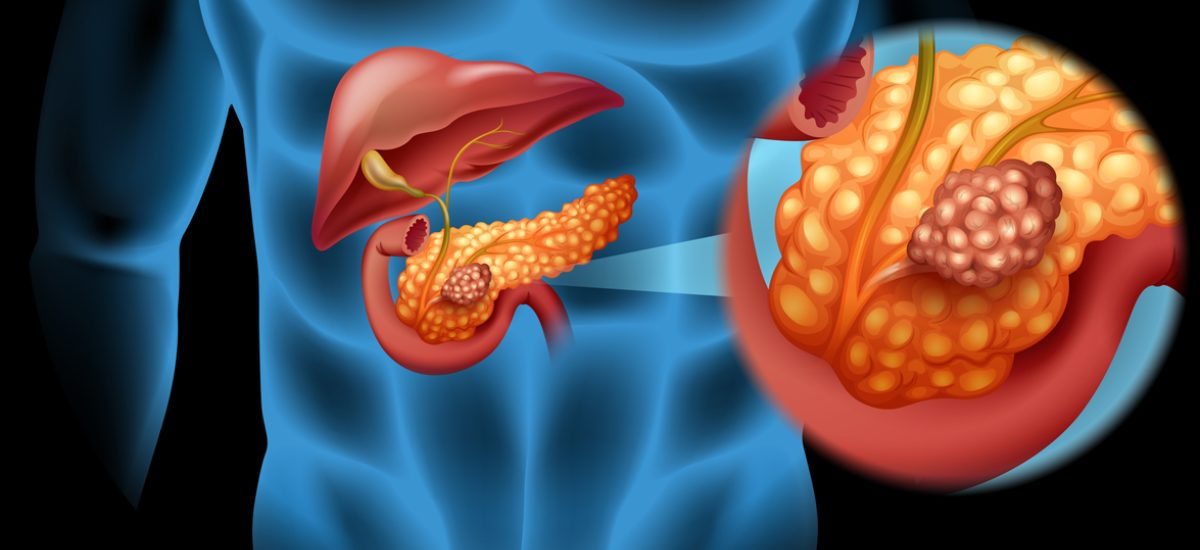
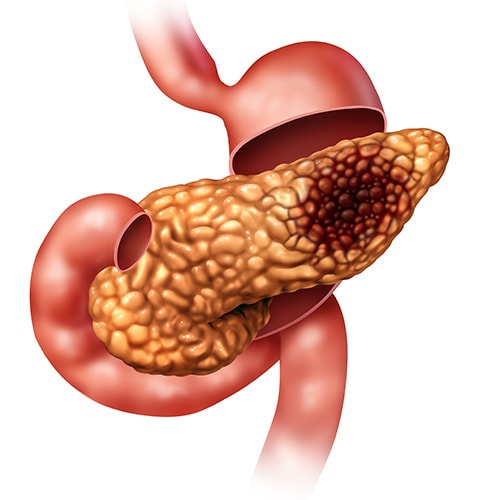
Pancreatic cancer is a disorder in which healthy cells in the pancreas cease to function properly and proliferate uncontrollably. These malignant cells can clump together and form a mass known as a tumor. A malignant tumor is one that can grow and spread to other regions of the body. A pancreatic tumor can disrupt pancreatic function, develop into neighboring blood arteries and organs, and eventually spread to other areas of the body through a process known as metastasis.
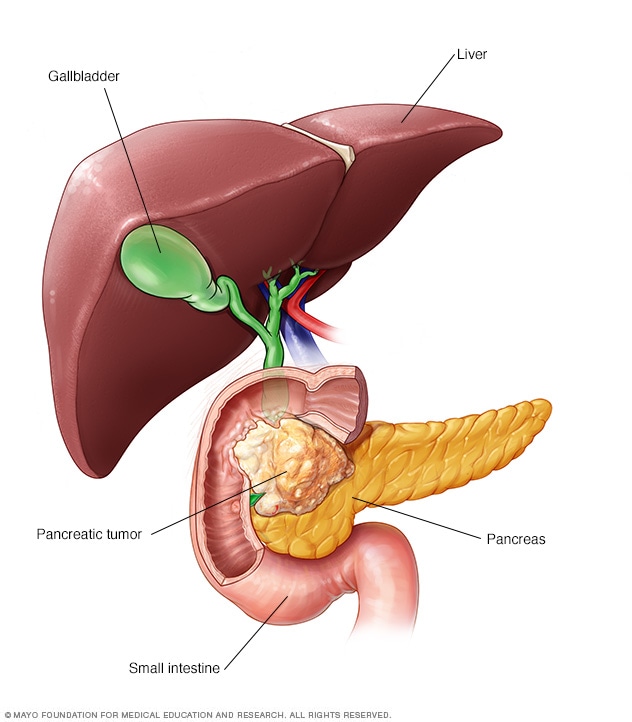
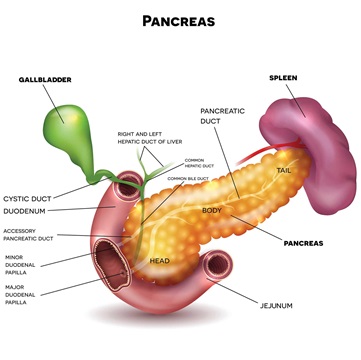
The pancreas is a pear-shaped gland positioned between the stomach and the spine in the center of the belly. It is made up of two major parts:
The exocrine component: consists of ducts and small sacs known as acini at the ends of the ducts. This section of the pancreas produces specific proteins known as enzymes, which are released into the small intestine to assist the body in digesting and breaking down food, particularly lipids.
The endocrine component: is made up of cells called islets of Langerhans that are clustered together in various locations within this section of the pancreas. These cells produce a variety of hormones, the most significant of which being insulin. Insulin is a hormone that regulates the quantity of sugar in the blood. Other hormones produced by this region of the pancreas include glucagon, somatostatin, pancreatic polypeptide (PP), and vasoactive intestinal peptide (VIP). Each of these hormones is crucial in controlling the body’s metabolism.
WHAT ARE THE TYPES OF PANCREATIC CANCER?
There are many forms of pancreatic cancer, based on whether the cancer started in the exocrine or endocrine component.
Exocrine tumors: This is the most frequent kind of pancreatic cancer. This form of cancer is commonly referred to as pancreatic cancer. Adenocarcinoma is the most frequent kind of exocrine malignancy. These tumors, known as ductal adenocarcinoma, frequently begin in the pancreatic ducts. Acinar adenocarcinoma is a far less common
type of tumor that starts in the acini.
The term “intraductal papillary mucinous neoplasm (IPMN)” refers to a type of cancer that is becoming more common. An IPMN is a tumor that forms within the pancreatic ducts and produces a thick fluid called mucin. The pancreatic ducts transport fluids from the pancreas to the colon to aid digestion. IPMN is not malignant when it first appears, but it has the potential to become cancerous if left untreated. By the time an IPMN is detected, it has often progressed to the stage of malignancy.
Acinar cell carcinoma, adenosquamous carcinoma, colloid carcinoma, giant cell tumor, hepatoid carcinoma, mucinous cystic neoplasms, pancreatoblastoma, serous cystadenoma, signet ring cell carcinoma, solid and pseudopapillary tumors, squamous cell carcinoma, and undifferentiated carcinoma are all much rarer types of
exocrine pancreatic tumors.
Endocrine tumors: PNETs (pancreatic neuroendocrine tumors) and islet cell tumors are other names for these. They are far less common than exocrine tumors, accounting for just around 7% of all pancreatic malignancies. This tumor is not the same as what most people think of as pancreatic cancer. A pancreatic neuroendocrine tumor can be active or inactive. Hormones are produced by a functional tumor. Hormones are not produced by a tumor that is not functioning. The hormone that the cells ordinarily produce is used to identify a functional neuroendocrine tumor. These are some examples:
WHAT ARE THE SIGNS AND SYMPTOMS OF PANCREATIC CANCER?
Pancreatic cancer patients may have the following symptoms or indicators. A symptom, such as weariness, nausea, or discomfort, is something that only the person experiencing it can identify and explain. A symptom is something that others can recognize and quantify, such as a fever, rash, or an increased pulse. Signs and symptoms, when combined, can assist describe a medical situation. People with pancreatic cancer may not exhibit any of the signs and symptoms listed below. Alternatively, the origin of a symptom or sign could be a medical disease other than cancer.
Doctors frequently refer to pancreatic cancer as a “silent illness” because there are few visible symptoms early on. Furthermore, there are currently no specific tests that may consistently detect cancer in patients who do not exhibit symptoms. When people do experience symptoms, they frequently resemble those of other medical disorders, such as an ulcer or pancreatitis. As the cancer progresses, the following symptoms may appear:
- Yellow skin (including the gums and inner lips) and/or eyes, darkening of the urine, itching, and clay-colored stool are all symptoms of jaundice caused by a bile duct obstruction.
- Upper abdominal pain, upper back pain, or arm pain
- Swelling of an arm or leg caused by a blood clot that is painful.
- Burning sensations in the stomach, as well as other gastrointestinal discomforts
- Floating stools with a particularly foul odor and an odd hue as a result of the body’s inability to metabolize fats
Please consult your doctor if you are concerned about any changes you are experiencing. In addition to other questions, your doctor will inquire as to how long and how frequently you have been experiencing the symptom(s). This is done to assist in determining the cause of the condition, which is referred to as a diagnostic.
If cancer is discovered, symptom relief is an important element of cancer care and treatment. This is known as “palliative care” or “supporting care.” It is frequently initiated shortly after diagnosis and continues throughout treatment. Make an appointment with your health care provider to discuss your symptoms, especially any new or changing symptoms. You may also wish to keep a written diary or notebook about your symptoms, complete with exact facts and dates, to help you communicate with your health care team.
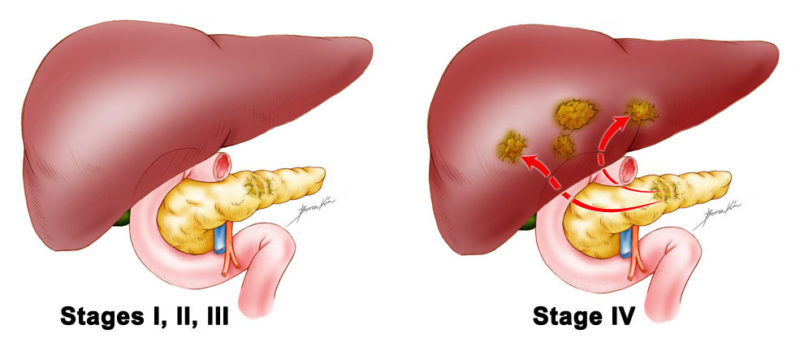
WHAT ARE THE STAGES OF PANCREATIC CANCER?
Staging describes where the cancer is present, whether or not it has spread, and whether or not it is impacting other sections of the body. Pathology and diagnostic reports often describe staging. Doctors utilize diagnostic tests to determine the stage of cancer, therefore staging may not be complete until all of the tests are completed. Knowing the stage allows the doctor to prescribe the best treatment, anticipate a patient’s prognosis, or possibility of recovery, and find clinical trials that may be treatment possibilities. Distinct forms of cancer have different stage descriptions. It is critical that the staging be performed at a medical center that has experience diagnosing and staging pancreatic cancer.
Pancreatic cancer is staged using a variety of methods. The “TNM classification,” which is used to stage other malignancies, is not commonly utilized to stage pancreatic cancer. However, it is described further below for completeness.
The more typical method of classifying pancreatic cancer is to divide a tumor into one of four groups based on whether it can be removed surgically and where it has spread:
- Resectable (localized): This kind of pancreatic cancer is surgically treatable. Surgery is frequently performed immediately following a diagnosis. Prior to surgery, further treatment may be necessary. The tumor may be only in the pancreas or it may extend beyond it, but it has not grown into any of the area’s major arteries or veins. There is no sign that the tumor has spread to other parts of the body than the pancreas. Approximately 10% to 15% of patients are diagnosed with this stage.
- Locally advanced: This type of pancreatic cancer is still only seen around the pancreas, but it cannot be surgically removed because it has spread into or near surrounding arteries, veins, or organs. This means that surgery cannot be used to remove it since the risk of injuring these nearby structures is too great. There is no evidence that it has spread to other parts of the body. This stage is diagnosed in approximately 35 percent to 40% of patients.
- Borderline resectable: This category represents a tumor that may be difficult or impossible to remove surgically when initially diagnosed, but if chemotherapy and/or radiation therapy may shrink the tumor first, surgery to remove the tumor with negative margins may be possible afterwards. A “negative margin” indicates that no visible cancer cells remain in the body.
- Metastatic: The tumor has spread from the pancreas to other organs such as the liver, lungs, or distant areas of the abdomen. This stage is diagnosed in approximately 45 to 55 percent of individuals.
The health care team can determine the optimum treatment strategy by categorizing each cancer into one of these categories.
TNM system of staging
System of TNM staging
Other forms of cancer are typically staged using a method known as the TNM system, which is used by doctors. During surgery, surgeons use this system to classify tumors. Many individuals with pancreatic cancer, however, do not have surgery. As a result, the TNM system is not as widely employed in pancreatic cancer as it is in other cancers.
Doctors use the results of diagnostic tests, scans, and surgery to answer the following questions for the TNM system:
- Tumor(T): What is the size of the main tumor? Where can I find it?
- Node(N): Has the cancer spread to your lymph nodes? If so, where and how many?
- Metastasis(M): Is the cancer in other parts of the body? If so, where and how much?
The results are aggregated to establish each person’s cancer stage. There are five stages: stage 0 (zero), stages I through IV (1 through 4). The stage provides a common language for doctors to describe the cancer so that they can collaborate to determine the best treatments. More information on each component of the TNM system for pancreatic cancer may be found below:
Tumor (T)
The “T” plus a letter or number (0 to 4) is used in the TNM system to describe the size and location of the tumor. The size of a tumor is measured in millimeters (cm). A centimeter is approximately the width of a normal pen or pencil.
The tumor stage assists the doctor in developing the most effective treatment plan for each patient. The information for each tumor stage is shown below.
TX: There is no way to analyze the original tumor.
T0: There was no sign of cancer in the pancreas.
Tis: This term refers to carcinoma in situ, which is a very early stage of cancer that has not spread.
T1: The tumor is only in the pancreas and is 2 centimeters (cm) or less in size. Based on the size of the tumor, this stage is further subdivided into T1a, T1b, and T1c.
T2: The tumor is only in the pancreas and is bigger than 2 cm but not bigger than 4 cm.
T3: The tumor is more than 4 centimeters in size and goes beyond the pancreas. It does not affect the major arteries or veins close to the pancreas.
T4: The tumor has spread beyond the pancreatic into major arteries or veins close to the pancreas. Surgery cannot entirely eradicate a T4 tumor.
Node (N)
The letter “N” in the TNM staging system refers to lymph nodes. As part of the body’s immune system, these small, bean-shaped organs distributed throughout the body aid in the battle against infection and disease. Regional lymph nodes are those near the pancreas and distant lymph nodes are those in other parts of the body in pancreatic cancer.
NX: The lymph nodes in the region cannot be examined.
N0: No cancer was discovered in the regional lymph nodes.
N1: The cancer has spread to one or more regional lymph nodes.
N2: The cancer has progressed to at least four regional lymph nodes.
Metastasis (M)
The “M” in the TNM system indicates if the cancer has migrated to other parts of the body, a condition known as metastasis.
M0: There has been no spread of the disease to other regions of the body.
M1: The cancer has progressed to a different portion of the body, including distant lymph nodes. Pancreatic cancer most usually spreads to the liver, the peritoneum (the lining of the abdominal cavity), and the lungs.
Cancer stage grouping
Doctors determine the cancer stage by integrating the T, N, and M classifications.
Stage 0: Cancer in situ, in which the cancer has not spread beyond the duct in which it began (Tis, N0, M0).
Stage IA: The tumor in the pancreas is 2 cm or less in size. It has not spread to the lymph nodes or any other sections of the body (T1, N0, M0).
Stage IB: The pancreas has a tumor that is larger than 2 cm in size. It has not spread to the lymph nodes or any other sections of the body (T2, N0, M0).
Stage IIA: The tumor is more than 4 cm in size and goes beyond the pancreas. It hasn’t migrated to neighboring arteries, veins, lymph nodes, or other organs (T3, N0, M0).
Stage IIB: A tumor of any size has not spread to adjacent arteries or veins. It has spread to one to three regional lymph nodes but has not moved to other areas of the body (T1, T2, or T3; N1; M0).
Stage III: Any of the following conditions:
- A tumor of any size that has spread to four or more regional lymph nodes but has not migrated to neighboring arteries, veins, or other bodily components (T1, T2, or T3, N2, M0).
- A tumor that has migrated to surrounding arteries and veins, as well as possibly to regional lymph nodes. It hasn’t spread to the rest of the body (T4, any N, M0).
Stage IV: Any cancerous tumor that has spread to other areas of the body (any T, any N, M1).
Recurrent: Cancer that recurs after therapy is referred to as recurrent cancer. If the cancer returns, more tests will be performed to determine the degree of the recurrence. These tests and scans are frequently comparable to those performed after the first diagnosis.
HOW IS PANCREATIC CANCER DIAGNOSED?
Many tests are used by doctors to detect or diagnose cancer. They also perform tests to see whether the cancer has spread to another place of the body from where it began. This is referred as as metastasis. Imaging tests, for example, can reveal whether or not the cancer has spread. Images of the inside of the body are produced via imaging tests. Doctors may also conduct tests to determine which treatments are most likely to be effective.
A biopsy is the only guaranteed way for a doctor to know if a part of the body has cancer in most cases of cancer. A cancer diagnosis, however, is also possible in the absence of a properly proven biopsy. During a biopsy, the doctor removes a small sample of tissue from the suspected cancerous spot for examination in a laboratory. Because of the position of the pancreas, biopsies for pancreatic cancer are notoriously difficult to perform. A biopsy is the only guaranteed way for a doctor to know if a part of the body has cancer in most cases of cancer. A cancer diagnosis, however, is also possible in the absence of a properly proven biopsy. During a biopsy, the doctor removes a small sample of tissue from the suspected cancerous spot for examination in a laboratory. Because of the position of the pancreas, biopsies for pancreatic cancer are notoriously difficult to perform.
Pancreatic cancer is diagnosed in the following ways:
There are numerous tests available to help diagnose pancreatic cancer. Not all of the tests outlined here will be utilized on every individual. When selecting a diagnostic test, your doctor may take the following variables into account:
- The cancer type suspected
- Your age, general health, and family history
- The outcomes of previous medical tests
If a doctor suspects a patient has pancreatic cancer, he or she will first inquire about the patient’s medical history and family history. The person will then be examined to search for evidence of the condition. It is critical to have an accurate and fast diagnosis. If at all possible, tests should be performed at a medical center that is familiar with the disease. When pancreatic cancer is suspected, the tests indicated below may be used. The diagnosis, however, should be verified by a sample of tumor tissue obtained during a biopsy, fine needle aspiration, or surgery. These tests are discussed in greater detail below.
General tests
- Physical examination: The doctor will check your skin, tongue, and eyes for yellowness, which is an indication of jaundice. Jaundice can be caused by a tumor in the head of the pancreas that prevents the normal flow of bile, which is produced in the liver. However, when pancreatic cancer is detected, many people do not have jaundice. Your doctor will also examine your belly for changes caused by the cancer, however the pancreas, which is positioned in the back of the upper abdomen, is rarely felt. Another indicator of cancer is an abnormal collection of fluid in the abdomen, known as ascites. The doctor will also examine your belly to see if you are experiencing pain in the top area of your abdomen, just behind your breast bone.
- Blood tests: Blood samples may be taken by the doctor to check for abnormal levels of bilirubin and other chemicals. Bilirubin is a substance that can accumulate in high quantities at people with pancreatic cancer due to tumor obstruction of the common bile duct. There are numerous non-cancerous causes of an increased bilirubin level, including hepatitis, gallstones, and a frequent virus known as mononucleosis, or “mono.” CA19-9 (carbohydrate antigen 19-9) is a tumor marker. A tumor marker is a chemical produced by a tumor that can be detected in the blood and may be found at higher levels if cancer is present. CA19-9 values are frequently elevated in pancreatic cancer patients, however some patients have normal CA19-9 levels. CA19-9 values frequently rise when the cancer progresses or spreads. CA 19-9 should not be used as the sole test to diagnose pancreatic cancer because elevated levels of CA 19-9 can also indicate other illnesses. Other tumors, such as colorectal, liver, and esophageal cancers, can raise CA 19-9 levels. Noncancerous diseases, such as pancreatitis, liver cirrhosis, and a noncancerous obstruction of the common bile duct, may also raise CA 19-9.
Imaging tests
Imaging tests assist doctors in determining the location of the cancer and whether it has migrated from the pancreas to other places of the body. Imaging examinations may also be done to track the progression of the malignancy. Because pancreatic cancer does not always manifest as a single huge tumor, it might be difficult to detect on imaging studies. Newer computed tomography scanners, on the other hand, offer better, clearer images that can aid in the detection of tumors. A radiologist is a physician who specializes in the interpretation of imaging tests.
- Computed tomography (CT) scan: A CT scan uses x-rays gathered from various angles to create images of the inside of the body. A computer combines these images to create a detailed multi-dimensional scan image (usually three dimensions or more) that shows any abnormalities or malignancies. A CT scan can be used to detect the size and location of the main tumor, as well as to assess the likelihood of metastasis to lymph nodes or other regions of the body. Typically, a specific dye known as a contrast medium is administered prior to the scan to improve image detail. This dye can be injected into a patient’s vein or given to them in the form of a pill or liquid to consume. A pancreatic protocol CT scan is a unique CT scan approach used by several cancer clinics. This procedure relies on photographing the pancreas at precise periods following an intravenous (IV) injection of contrast material to determine the exact location of the tumor in relation to surrounding organs and blood arteries. The findings of this test can assist determine whether the tumor can be removed surgically. ASCO advises persons with metastatic pancreatic cancer to have a CT scan of their chest, abdomen, and pelvis to determine the extent of the malignancy. A CT scan or other imaging may also be performed to monitor therapy success 2 to 3 months after conventional treatment begins.
- Positron emission tomography (PET) scan or PET-CT scan: A PET scan is frequently coupled with a CT scan, resulting in a PET-CT scan. It is sometimes paired with MRI. However, your doctor may refer to this technique simply as a PET scan. A PET scan is a technique for producing multi-colored images of organs and tissues within the body. A tracer, which is a radioactive sugar compound, is delivered into the patient’s bloodstream in small amounts. Fluorodeoxyglucose is the most often used tracer in pancreatic cancer PET studies (FDG). This sugar substance is absorbed by the cells that consume the most energy. Cancer absorbs more of the radioactive tracer chemical because it uses energy actively. The amount of radiation in the material, on the other hand, is purposefully created to be too low to be hazardous. This material is then detected by a PET scanner, which produces images of the inside of the body. The combination provides a more comprehensive picture of the area under consideration. A PET scan should never be utilized in place of a high-quality, fast CT scan. PET scans are distinct from CT scans in that CT scans examine the tumor in respect to your anatomy, whereas PET scans seek to evaluate metabolic activity.
- Endoscopic retrograde cholangiopancreatography (ERCP): A gastroenterologist performs this technique. The doctor will insert a narrow, illuminated tube called an endoscope into the small intestine through the mouth and stomach. The endoscope is then used to guide a tiny tube called a catheter into the bile and pancreatic ducts. Dye is injected into the ducts, and x-rays are taken to determine whether a duct is squeezed or narrowed. During ERCP, a plastic or metal stent can often be inserted across the clogged bile duct to help relieve any jaundice. During this process, tissue samples can be collected, which can sometimes aid confirm a cancer diagnosis. During this operation, the patient is only mildly sedated. ERCP is most typically used to insert bile duct stents and is rarely utilized for diagnosis.
- Ultrasound: An ultrasound creates a picture of the interior organs by using sound waves. Ultrasound devices are classified into two types:
-
- The doctor places a transabdominal ultrasound instrument on the outside of the belly and slowly moves it around to generate an image of the pancreas and surrounding structures.
-
- Endoscopic ultrasound (EUS) is a narrow, illuminated tube that is passed through the patient’s mouth, stomach, and small intestine. It is carefully moved around the area to photograph the pancreatic. This treatment is highly specialized and necessitates the services of a gastroenterologist with advanced expertise in this field. A gastroenterologist is a doctor who specializes in the digestive tract, which includes the stomach, intestines, and other comparable organs. EUS is usually performed while the patient is sedated, so he or she sleeps through the operation. A biopsy may also be performed concurrently with this technique.
Percutaneous transhepatic cholangiography (PTC): A tiny needle is introduced through the skin and into the liver during this x-ray treatment. A dye is injected through the needle, causing the bile ducts to be seen on x-rays. The doctor can identify if the bile ducts are blocked by looking at the x-rays.
Magnetic resonance imaging (MRI): An MRI produces detailed images of the body by using magnetic fields rather than x-rays. The tumor’s size can be determined via an MRI. To provide a crisper image, a special dye known as a contrast medium is administered before to the scan. This dye can be injected into a patient’s vein or given to them in the form of a pill or liquid to consume. Magnetic resonance cholangiopancreatography (MRCP) is a type of MRI that uses computer software designed specifically to look for pancreatic abnormalities such ductal obstructions and cysts.
Biopsy and tissue tests
- Biopsy: A biopsy is the removal of a small sample of tissue for microscopic examination. Other tests can indicate the presence of cancer, but only a biopsy can provide a definitive diagnosis for most malignancies. The material is next examined by a pathologist (s). A pathologist is a medical professional who specializes in interpreting laboratory tests and assessing cells, tissues, and organs to identify disease. In the case of pancreatic cancer, the pathologist may have specific experience examining pancreatic cancer biopsy samples. There are two methods for obtaining a tissue sample:
-
- Fine needle aspiration (FNA): An FNA suctions out cells using a fine needle introduced into the pancreatic. This is usually done using an EUS or via the skin, which is called percutaneously, and is guided by a CT scan.
-
- Biopsy with a core needle: This is utilized to obtain a bigger portion of tissue that can be used for biomarker or genetic testing of the tumor. A core biopsy, on the other hand, carries more hazards than a FNA, such as pancreatitis and bleeding. It should be performed by a gastroenterologist who has received special training and has extensive experience with EUS.
If the cancer has progressed to other organs, a biopsy from one of these sites, such as the liver, may be required. Again, this can be done through the skin, as previously mentioned, or by surgery, which is less common. This sort of surgery can be performed via a bigger incision in the belly known as a laparotomy. A laparoscopic method, which uses considerably smaller incisions to provide openings for a tiny camera and surgical instruments, can also be used.
A biopsy may occasionally reveal that there are no cancer cells in the area investigated, even if there are. This is known as a “false negative.” This can happen because the area has inflammation and/or fibrosis (scar-like tissue), which can make it difficult to locate cancer cells. In general, before a patient begins therapy, every effort is done to confirm the presence of cancer, even if this necessitates numerous biopsies. Patients with a tumor in a specific location of the pancreas that can be removed surgically, even if a biopsy is not conducted or the biopsy does not reveal cancer cells, are an exception.
- Molecular, or biomarker, testing of the tumor: Additional molecular tests on the tumor sample may be recommended by your doctor, and you may request them, to discover particular mutations, genetic abnormalities, protein expression, and other molecular traits unique to the tumor. Some of these tests can be performed at the laboratory of your local hospital. Other tests may necessitate sending the material to an independent laboratory for analysis.
Molecular testing should be undertaken to look for evidence of high microsatellite instability (MSI-high) or defective mismatch repair (dMMR); for mutations in the BRCA gene, as well as other genes involved in DNA damage repair; and for an NTRK fusion. These tests may assist doctors in determining your treatment options, which may include immunotherapy and targeted therapy. These results, however, are uncommon in pancreatic cancers. It’s also worth noting that these findings can take weeks to come in, and you don’t have to wait for them before commencing therapy.
Molecular testing is also known as “targeted therapy testing,” “personalized medicine,” “precision medicine,” or “next generation sequencing.” This field of science and treatment is quickly expanding, with increased interest, scientific focus, and research progress. It is beneficial to learn about the type and amount of tumor sample required for these tests, as well as if they are covered by your health insurance. Another biopsy may be required to get a large enough tissue sample for more detailed examination. A blood test, depending on the type of testing, can provide information on some of the molecular or genetic aspects of your cancer.
Discuss with your doctor the possible information that tests like drug assays could provide to help plan your treatment, as well as whether such tests are covered by your insurance.
People who have surgery may also choose to contribute tumor fragments that are no longer needed for their diagnosis or cancer therapy so that the samples can be utilized to advance pancreatic cancer research.
- Germline testing: It is currently advised that all persons with a pancreatic cancer diagnosis undergo germline testing. This entails looking for mutations in a person’s DNA that may suggest a hereditary propensity to cancer in a blood or saliva sample. This is usually done in conjunction with a visit to a genetic counselor. If a person is discovered to be a carrier for specific genetic mutations, this information may assist guide treatment decisions if pancreatic cancer is identified. It would also indicate that their family members should pursue genetic testing and joining a pancreatic cancer family registry.
Following the completion of diagnostic testing, your doctor will discuss the results with you, including the specific type of cancer you have, the extent to which the disease has grown and spread (referred to as the stage), and your treatment options. You may obtain copies of all test results and photos for your personal records.
WHAT ARE THE TREATMENTS OF PANCREATIC CANCER?
When deciding on a treatment strategy, you should consider clinical trials as an alternative. A clinical trial is a research study that puts a new therapeutic strategy to the test. Doctors want to know if the new treatment is safe, effective, and possibly superior than the traditional treatment. Clinical trials can be used to evaluate a novel drug, a new combination of standard treatments, or new doses of standard pharmaceuticals or other treatments. Clinical trials are an option to consider for cancer therapy and care at all stages. Your doctor can assist you in considering all of your treatment options.
How is Pancreatic Cancer Treated?
Different types of doctors and other health care providers frequently collaborate in cancer care to construct a patient’s overall care and treatment plan, which combines various types of treatments and supportive care. This is referred to as a multidisciplinary team. Other health care professionals on cancer care teams include physician assistants, nurse practitioners, oncology nurses, patient navigators, social workers, pharmacists, counselors, nutritionists, and others.
The most prevalent types of pancreatic cancer treatments are given here, followed by a general overview of treatments by stage. Pancreatic cancer treatment options currently include surgery, radiation therapy, chemotherapy, targeted therapy, and immunotherapy. Your treatment plan will also include treatment for symptoms and side effects, which is an important aspect of cancer care.
The type and stage of cancer, potential side effects, and the patient’s preferences and overall health all influence treatment options and recommendations. Take the time to read about all of your treatment options, and don’t be afraid to ask clarifying questions. Discuss the aims of each treatment with your doctor, as well as what you can expect during treatment. These discussions are known as “shared decision-making.” When you and your doctors collaborate to identify therapies that meet the goals of your care, this is referred to as shared decision-making. Because there are various treatment choices for pancreatic cancer, shared decision-making is very vital.
Pancreatic cancer has a far better chance of being effectively treated if found early. However, for individuals with advanced pancreatic cancer, there are medicines that can help control the disease and allow them to live longer and more comfortably.
Surgery
Depending on the location and size of the tumor in the pancreas, surgery for pancreatic cancer may involve removing all or part of the pancreas. An region of healthy tissue surrounding the tumor is frequently removed as well. This is known as a margin. The goal of surgery is to have “clean margins” or “negative margins,” which means no cancer cells in the boundaries of the healthy tissue removed.
A surgical oncologist is a specialist who specializes in the surgical treatment of cancer.
Because most pancreatic cancers are discovered after the disease has spread, only around 20% of those diagnosed are able to receive surgery. When surgery is a prospective treatment option, there are numerous factors to consider before undergoing such a procedure. Before deciding on surgical therapy, you should have a detailed discussion with your health care team, especially a pancreatic surgical oncologist. This discussion should involve discussing the advantages, disadvantages, and recovery time of the specific procedure chosen for you. If surgery is not an option, you and your doctor will discuss alternative treatments. For less frequent diseases, such as pancreatic cancer, it is normal to obtain a second opinion from a skilled surgical oncologist.
Pancreatic cancer surgery may be paired with systemic therapy and/or radiation therapy. These additional therapies are typically administered following surgery, and are referred to as adjuvant therapy. However, systemic and/or radiation therapy may be utilized prior to surgery to decrease a tumor. This is known as neoadjuvant or pre-operative therapy. Before surgery, the tumor is re-staged following neoadjuvant therapy. Another CT scan is frequently used for re-staging to look at the change in tumor size as well as what surrounding tissues and blood vessels it is affecting.
Depending on the objective of the surgery, different types of surgery are performed.
- Laparoscopy: The surgeon may choose to begin with a laparoscopy in some cases. Several small holes are created in the abdomen during a laparoscopy, and a tiny camera is inserted into the body while the patient is sedated. Anesthesia is a drug that helps to inhibit the perception of pain. During this procedure, the surgeon will be able to determine whether the cancer has spread to other sections of the abdomen. If it has, surgery to remove the primary pancreatic tumor is generally not advised.
- Surgery to remove the tumor: Depending on where the tumor is located in the pancreas, several forms of surgery are performed. All of the operations listed below include the removal of adjacent lymph nodes as part of the procedure. In most cases, more than one type of surgeon, as well as other specialists, will be involved in your procedure.
-
- Whipple procedure: This surgery is also referred to as a pancreaticoduodenectomy. If the cancer is only in the head of the pancreas, a Whipple procedure may be performed. This is a major operation in which the surgeon removes the pancreas head and a section of the small intestine called the duodenum, as well as the bile duct and stomach, or sometimes simply a portion of the stomach. The surgeon next reattaches the digestive tract and biliary system. Temporary drains are typically placed in the belly to aid in drainage and patient recovery. Drains are typically implanted after surgery and kept in place afterward to drain any pancreas juice leakage to the outside of the body. Drains are left in place for varying amounts of time depending on the amount and nature of their output, however they can be removed while still in the hospital and can remain in place for up to 2 to 3 months. This treatment should be performed by a surgeon who has experience treating pancreatic cancer. The Whipple technique is available in numerous forms, including routine, pylorus-preserving, and radical pancreaticoduodenectomy.
-
- Distal pancreatectomy: This procedure is often performed if the malignancy is found on the left side of the pancreas’ tail. The tail and body of the pancreas, as well as the spleen, are removed during this surgery.
-
- Total pancreatectomy: If the cancer has spread throughout the pancreas or is found in many locations, a total pancreatectomy may be required. The entire pancreas, a portion of the small intestine, a portion of the stomach, the common bile duct, the gallbladder, and the spleen are removed during a total pancreatectomy.
To aid with symptoms that are affecting a patient’s quality of life, supportive surgery and palliative operations are frequently prescribed. Palliative therapies and surgeries can include bypass surgery, stent placements, and nerve blocks to treat jaundice, nausea, vomiting, and tumor-related pain.
You will be required to stay in the hospital following surgery. The length of your hospital stay will be dictated by the sort of surgery you’ve had, although it might range from several days to several weeks or longer. It will also contain a plan for at-home rest and rehabilitation. At-home rest could last a month or more, with full recovery taking around two months. Your health care team will collaborate closely with you on your pre-surgical preparation and post-surgery recovery plans, which will include vital exercise, drain management (if a drain is placed during surgery), mindfulness, and dietary and nutritional advice.
For the first several weeks after surgery, patients may experience weakness, weariness, and pain. Other negative effects of pancreas removal include trouble digesting food and diabetes due to the absence of insulin produced by the pancreas. Before surgery, discuss with your health care team the potential side effects of the specific surgery you’ll be having and how they can be controlled.
Radiation therapy
The use of high-energy x-rays or other particles to eliminate cancer cells is known as radiation therapy. A radiation oncologist is a doctor who specializes in the use of radiation therapy to treat cancer. External-beam radiation therapy, which delivers radiation from a machine outside the body, is the most prevalent method of radiation treatment.
External-beam radiation therapy is the most often utilized method of radiation therapy for pancreatic cancer. A radiation therapy regimen, or schedule, typically consists of a predetermined number of treatments administered over a predetermined time period. Radiation can be used in a variety of ways.
- Traditional radiation therapy: This is also known as standard fraction radiation therapy or conventional fraction radiation therapy. It consists of daily treatments of reduced radiation doses each fraction or day. It is typically administered over the course of 5 to 6 weeks, with weekends off from treatment.
- SBRT (stereotactic body radiation) or cyberknife: These are shorter treatments of greater doses of radiation therapy that can be completed in as little as 5 days. This is a newer type of radiation therapy that can deliver more targeted treatment in fewer sessions. It is unknown whether this strategy performs as well as regular radiation therapy, and it may not be appropriate for everyone. It should only be administered at specialized centers with experience and skill in administering this technology for pancreatic cancer and determining who will benefit the most from it.
- Proton beam therapy: This is an external-beam radiation therapy technique that use protons rather than x-rays. Protons have the ability to destroy cancer cells at high energies. It also reduces the amount of radiation that reaches healthy tissue. Proton beam therapy can be administered for a set period of time or for a shorter period of time, similar to SBRT. It is unknown whether it is more effective than regular radiation therapy, and it may not be suitable for everyone. It should be administered in treatment centers that have the necessary competence and skills to administer this treatment for pancreatic cancer, which may only be offered through a clinical trial.
Other types of radiation therapy may be available. Radiation therapy can be administered in a variety of methods, so it’s critical to discuss your options with your doctor.
Chemotherapy is frequently administered concurrently with radiation therapy because it might improve the effects of the radiation therapy, a process known as radiosensitization. Combining chemotherapy and radiation therapy may help reduce the tumor sufficiently for it to be removed surgically on occasion. Chemotherapy performed concurrently with radiation therapy, on the other hand, frequently requires lower dosages than chemotherapy given alone.
Radiation therapy may be beneficial in lowering the chance of pancreatic cancer returning or regrowing in the initial site. However, it is unclear how much, if any, it increases a person’s life expectancy.
Radiation therapy side effects may include fatigue, moderate skin responses, nausea, upset stomach, and loose bowel motions. The majority of negative effects fade quickly after treatment is completed. Discuss what you should expect and how side effects will be addressed with your health care team.
Chemotherapy
Chemotherapy is the use of medications to eradicate cancer cells, typically by preventing the cancer cells from growing, dividing, and proliferating.
A chemotherapy regimen, or schedule, typically consists of a predetermined number of cycles administered over a predetermined time period. In between cycles, there is normally a rest time. A patient may be administered one medicine at a time or a mixture of drugs at the same time. The U.S. Food and Drug Administration (FDA) has approved the following medications for pancreatic cancer:
- Fluorouracil (fluorouracil) (5-FU)
- Nab-paclitaxel (Abraxane)
- Nanoliposomal irinotecan (Onivyde)
Combination therapy are usually best for persons who can carry out their normal daily activities without assistance. This is due to the fact that when two or more medications are used concurrently, the adverse effects are often more severe.
The choice of which combination to utilize varies depending on the patient’s unique diagnosis, stage of disease, treatment history, genetic composition, side effects, and overall health. Other factors that can have an impact include the cancer center and the oncologist’s experience with the medications. Chemotherapy for pancreatic cancer can be defined by when and how it is administered:
- First-line chemotherapy: This is usually the first treatment given to those who have either locally advanced or metastatic pancreatic cancer and have not previously received treatment.
- Second-line chemotherapy: When the first treatment fails or ceases to suppress cancer growth, the cancer is referred to as “refractory.” When first-line treatment fails, this is referred to as primary resistance. Alternatively, medication may be successful for a period of time before ceasing to be effective, a condition known as secondary or acquired resistance. In these cases, if the patient’s overall health is good, he or she may benefit from extra treatment with various medications. There is extensive ongoing research focused on creating novel medicines for second-line, third-line, and beyond treatment. Some of these have shown a lot of potential.
- Off-label use: This is when a medicine is prescribed for a condition that is not stated on the label. This signifies that the drug is not being used to treat the condition(s) for which it has been officially approved by the FDA. It could also imply that the medication is being administered in a manner that differs from the recommendations on the label. As an example, suppose a doctor wants to use a medicine that has only been approved for breast cancer to treat pancreatic cancer. Off-label use of a drug is only advised when there is strong evidence that the drug may be effective for a disease that is not included on the label. This evidence could include previously published studies, promising outcomes from ongoing research, or results from tumor biomarker tests that indicate the medicine may function. Off-label drug use, on the other hand, may not be reimbursed by your health insurance carrier. There may be exceptions, but it is critical that you and/or your health care team consult with your insurance provider before beginning this sort of treatment.
Chemotherapy side effects
The adverse effects of chemotherapy vary depending on the medications used. Furthermore, even when given the same treatment, not all patients experience the same adverse effects. In general, side effects may include a loss of appetite, nausea, vomiting, diarrhea, gastrointestinal issues, rash, mouth sores,
hair loss, and fatigue. Chemotherapy patients are also more likely to have low levels of white blood cells, red blood cells, and platelets, which puts them at a higher risk of anemia, infections, and easily bruising and bleeding.
Certain pancreatic cancer medicines have also been associated to specific side effects. Capecitabine, for example, can produce redness and irritation on the palms of the hands and soles of the feet. This is known as hand-foot syndrome. Oxaliplatin can produce peripheral neuropathy, which is characterized by cold sensitivity, numbness, and tingling in the fingers and toes. Peripheral neuropathy is another negative effect of nab-paclitaxel. These are just a few examples, and it is critical to discuss the side effects of the cancer medication(s) advised for you with your doctor ahead of time.
Most adverse effects fade away between treatments and when they are completed, but others can be long-lasting and increase as therapy progresses. Your doctor can advise you on how to alleviate these adverse effects. If the side effects are severe, your doctor may reduce the chemotherapy dose or temporarily stop the treatment.
Targeted therapy
Targeted therapy is a type of cancer treatment that targets specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. This method of treatment inhibits cancer cell growth and spread while limiting damage to healthy cells.
The targets of all cancers are not the same. Your doctor may order tests to determine the genes, proteins, and other variables in your tumor in order to find the most effective treatment. This enables clinicians to provide the most effective treatment to each patient whenever possible. Furthermore, research studies are continuing to learn more about specific molecular targets and new treatments aimed at them.
- Erlotinib (Tarceva): The FDA has approved this medicine in combination with the chemotherapy treatment gemcitabine for persons with advanced pancreatic cancer. Erlotinib inhibits the action of the epidermal growth factor receptor (EGFR), a protein that can become aberrant and aid in the formation and spread of cancer. This medication is taken orally by mouth as a pill, usually once a day. Erlotinib side effects include acne-like skin rash, diarrhea, loss of appetite, and weariness.
- Olaparib (Lynparza): This medication is approved for persons who have advanced pancreatic cancer with a germline (hereditary) BRCA mutation. It is designed for use as maintenance therapy after a patient has completed at least 16 weeks of platinum-based chemotherapy, such as oxaliplatin or cisplatin, with no indication of disease progression. This medication is taken orally by mouth as a pill, usually twice a day. Nausea, vomiting, diarrhea, or constipation, exhaustion, dizziness, lack of appetite, taste changes, low red blood cell counts, low white blood cell counts, gut discomfort, and muscle and joint pain are all common adverse effects of this medication.
- Larotrectinib (Vitrakvi) and entrectinib (Rozlytrek): These are tumor-agnostic drugs that can be used to treat any form of cancer that has a specific genetic alteration known as an NTRK fusion. This type of genetic alteration can be discovered in a variety of tumors, including pancreatic cancer, but it is uncommon. It is approved as a treatment for metastatic or locally advanced pancreatic cancer that has not responded to chemotherapy. This medication is taken orally as a tablet, usually once or twice a day. Dizziness, lethargy, nausea, vomiting, constipation, weight gain, and diarrhea are all common adverse effects.
Discuss with your doctor the potential side effects of a certain medicine and how to manage them.
Immunotherapy
Immunotherapy, also known as biologic therapy, is intended to increase the body’s natural defenses against cancer. It employs components created by the body or in a laboratory to enhance, target, or restore
immune system activity.
Immune checkpoint inhibitors, such as anti-PD-1 antibodies pembrolizumab (Keytruda) and dostarlimab (Jemperli), are a treatment option for pancreatic tumors with high microsatellite instability (MSI-H) or mismatch repair deficiency (dMMR). High MSI-H is related with approximately 1% to 1.5 % of pancreatic malignancies.
Immunotherapy in combination with chemotherapy is also being investigated in new clinical trials.
Different forms of immunotherapy might result in a variety of adverse effects. Consult your doctor about the potential adverse effects of the immunotherapy that has been prescribed for you.
Metastatic pancreatic cancer
Metastatic cancer occurs when cancer spreads to a different place of the body than where it began. If this occurs, it is advisable to consult with specialists who have treated similar cases in the past. Different doctors may have differing views on the optimal conventional treatment strategy. Clinical trials may potentially be a possibility, so speak with your doctor about clinical trials that you could be eligible for. Learn more about getting a second opinion before beginning treatment so that you are confident in your treatment plan.
Your treatment strategy may contain a combination of the above-mentioned treatments. Treatment options for patients with metastatic pancreatic cancer are highly influenced by a patient’s overall health, preferences, and support network.
First-line alternatives, depending on your preferences, characteristics, and comorbidity profile, include:
- FOLFIRINOX, which is a chemotherapy that combines fluorouracil, leucovorin, irinotecan, and oxaliplatin.
- Gemcitabine in combination with nab-paclitaxel.
- For patients who are not in good enough health to tolerate the more aggressive combinations described above, gemcitabine can be used alone.
- Another gemcitabine- or fluorouracil-based combination, such as gemcitabine plus cisplatin, gemcitabine plus capecitabine, or FOLFOX, may be utilized on occasion.
Those listed below are examples of second-line choices. These are typically used when a patient’s ailment progresses or when they experience severe side effects from first-line medication.
- Based on the patient’s general health and shared decision-making, fluorouracil alone or in combination with nanoliposomal irinotecan, irinotecan, or oxaliplatin may be advised.
- Gemcitabine may be given alone or in combination with nab-paclitaxel.
- When the cancer has high microsatellite instability (MSI-high) or a mismatch repair defect, pembrolizumab is recommended (dMMR). It is crucial to emphasize that MSI-high illness affects only about 1% of persons with pancreatic cancer.
- Any cancer with an NTRK fusion should be treated with larotrectinib or entrectinib. NTRK fusions are extremely uncommon in pancreatic cancer.
- Patients with a hereditary BRCA1 or BRCA2 mutation who have had first-line platinum-based chemotherapy that has stopped the cancer from growing or spreading for 16 weeks or more may continue treatment with chemotherapy or olaparib, a targeted medication. Maintenance therapy is a treatment that aims to keep the cancer in remission and is an option following a joint decision-making process between the patient and clinician.
Maintenance therapy may also be an option for patients whose disease has not progressed on first-line treatment but who are unable to continue with their previous treatment due to side effects. Following first-line platinum-based chemotherapy, the sole approved maintenance therapy is olaparib, which is effective in persons with metastatic pancreatic cancer coupled with a germline (hereditary) BRCA mutation. Other people may benefit from maintenance therapy by simplifying their first chemotherapy course. For example, gemcitabine/nab-paclitaxel could be reduced to gemcitabine alone, or FOLFIRINOX could be reduced to FOLFOX, FOLFIRI, or capecitabine.
Supportive care, often known as palliative care, will be necessary to alleviate symptoms and adverse effects. Discuss your symptoms, your mental health, and the social support available to you with your doctor as soon as possible. Treatment will be provided to alleviate any cancer-related pain or other symptoms.
A diagnosis of metastatic cancer can be extremely stressful and traumatic for many people. You and your family are encouraged to express your feelings to doctors, nurses, social workers, and other members of the health care team. Talking with other patients, such as in a support group or other peer support program, may also be beneficial.